Figure 1.
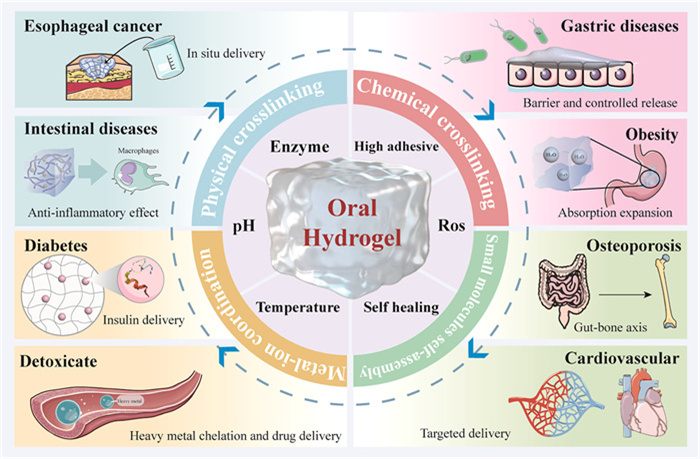
Scheme view of the review.
Recent advances in oral hydrogel drug delivery system for disease treatment
Peishuang Yu , Bohan Chen , Bingyu Xie , Mengjiao Zhou , Chengying Wang , Shenshen Yang , Wei Huang , Yubo Li

In recent years, increasing attention has focused on the "dose-effect" relationship of drugs, emphasizing drug safety and potential adverse reactions. Many traditional Chinese medicines, along with their active ingredients, and synthetic compounds often exhibit low bioavailability, requiring repeated high dosages to achieve therapeutic effects. This practice increases patient burden and elevates the risk of adverse reactions. Oral drug administration remains preferable due to its convenience and patient compliance, making oral drug delivery systems a prominent research area. Hydrogels are hydrophilic polymer materials characterized by three-dimensional networks capable of swelling without dissolving in water. Their similarity to the extracellular matrix confers excellent biocompatibility and biodegradability, making hydrogels widely applicable in biomedical fields [1-3]. In recent years, the administration mode of hydrogels has also changed from external dressing and in-situ injection to oral administration. For example, Liu et al. [4] describe drug formulations based on liquid in situ-forming tough hydrogels, that form directly in the stomach, thereby protect drugs, therapeutic enzymes, and beneficial bacteria in the hydrogels from stomach acid destruction. Furthermore, hydrogels can incorporate iohexol or cerium oxide to serve as scanning contrast agents for gastrointestinal (GI) inflammation, while cerium oxide also plays an anti-inflammatory and anti-fibrosis role [5,6]. Engineered Escherichia coli encapsulated within hydrogels has also been utilized as a non-invasive diagnostic tool to assess intestinal inflammation progression [7]. As an innovative drug delivery platform, oral hydrogels, with its outstanding biocompatibility, precise drug release control, and excellent drug protection ability, overcomes the problems of drug leakage, burst release, poor biocompatibility, and degradation faced by traditional drug delivery systems, and provides more possibilities for future drug treatment [8,9].
With the deepening of research and the continuous progress of technology, oral hydrogels will be more and more widely used in the drug delivery, offering the potential to enhance therapeutic outcomes, reduce side effects, and enable personalized medicine. This review focuses on the latest developments in the oral hydrogel system for the treatment of various diseases. The overall schematic diagram of this review is shown in Fig. 1. Firstly, the physiological factors of GI tract and the matrix materials of oral hydrogel delivery system are discussed. Then, its design strategy is introduced, including physical crosslinking, chemical crosslinking, small molecule self-assembly, and metal ion coordination. Moreover, the research strategy of oral intelligent hydrogel system and drug loading mode was summarized. Finally, the application of oral hydrogels in the treatment of various diseases in recent years is reviewed to provide a valuable reference for the development of hydrogel drug delivery systems.
Oral administration has become a new development direction of hydrogels in disease treatment due to its advantages of high patient compliance, easy access to drugs, and portability. In this section, we focus on the design strategies of oral hydrogel delivery systems, highlighting how hydrogel formation mechanisms, responsiveness to the GI microenvironment, and different drug loading strategies.
Some clinical drug administration methods each have strengths and limitations. Injections offer high bioavailability, but may cause pain and infection risk [10]. Transdermal administration is easy to operate, but has limited absorption and potential for skin irritation [11]. Rectal administration directly targets rectal diseases, but suffers from low patient acceptance and limited dosage forms [12]. Oral administration is usually preferred administration due to its convenience, high patient acceptance, and suitability for long-term treatment. However, oral administration still faces some physiological barriers in the GI tract. (1) The highly acidic environment of the stomach (pH 1.5–1.9) and abundant digestive enzymes may lead to the degradation of drugs in the stomach [13]. (2) The pH value, digestive enzymes, and transport proteins in different parts of the intestine may vary, thereby affecting the absorption efficiency of drugs in the intestine. (3) The physical barrier of intestinal mucosa, microbial metabolism, drug solubility, and transport time all affect the bioavailability of drugs [14,15].
Because of its high molecular weight and three-dimensional cross-linked network structure, oral hydrogels are usually not directly absorbed by the GI tract, but play the role of drug delivery platform in situ in the digestive tract. They typically release drugs in the target area through mechanisms such as swelling diffusion and environmentally responsive disintegration [16]. The released drug can be absorbed by the intestinal epithelium and enter the bloodstream, or directly exert anti-inflammatory and anti-tumor effects in local areas such as the colon, stomach, and intestines. The hydrogel system based on chitosan (CS), hyaluronic acid (HA), gelatin, etc. also has good biological adhesion and tissue retention ability, which can extend the action time in the focus area and enhance the efficacy [17,18]. Several studies on fluorescence tracking and tissue distribution in vivo have confirmed that the hydrogels will gradually degrade after drug release or be discharged from the body with intestinal peristalsis, without causing accumulation or systemic toxicity [19,20].
Oral hydrogels have various drug release mechanisms, including physical and chemical processes such as diffusion, swelling, degradation and chemical bond breaking. Among them, diffusion control is the most common mechanism, and drugs are gradually released through the pores of the hydrogel network; the swelling control mechanism depends on the looseness of the network structure of the hydrogels after water absorption and expansion, and is often used together with the pH responsive mechanism to promote drug extravasation [21]. In addition, some biodegradable hydrogels can be slowly degraded in the GI environment to achieve continuous release [22]. In recent years, intelligent responsive hydrogels have been widely studied, which can respond to pathological signals such as enzyme environment, temperature or oxidative stress in the GI tract to achieve site specificity and focus targeted release [23]. Multi mechanism synergistic regulation becomes one of the key strategies to improve the release efficiency and therapeutic targeting of oral hydrogels.
The structural stability of hydrogels in oral drug delivery systems depend to a large extent on the selected matrix materials. At present, the materials commonly used to construct oral hydrogels are mainly divided into three categories: Natural polymers, synthetic polymers and self-assembled small molecular materials. The three have their own characteristics in material sources, structural control ability and biological behavior.
Natural polymers originate from living organisms and have diverse structures. They are highly valued for their excellent biocompatibility, biodegradability, and low toxicity. Representative materials include sodium alginate (SA), CS, HA, inulin, etc. [24,25]. The advantages of natural polymers lie in their wide range of sources, mild structure, and suitability for encapsulating bioactive substances; but there are also problems such as uneven molecular structure and low mechanical strength, which have certain limitations in some systems that require precise structural control.
Synthetic polymer materials, such as polyethylene glycol, polyacrylic acid (PAA), have highly controllable chemical structure and gelling behavior, and can achieve fine adjustment of hydrogel performance by adjusting molecular weight, cross-linking density and functional group modification [26-28]. It has excellent mechanical properties and high gel strength, making it suitable for loading high concentration drugs or constructing complex structures for oral delivery. The outstanding advantage of synthetic polymers lies in their strong controllability and suitability for industrial preparation; however, some monomers or crosslinking agents have potential toxicity risks, and it is necessary to strictly optimize the synthesis route and remove residues to ensure the safety of oral use.
In recent years, self-assembled small molecule materials have emerged, including polyphenols, and drug derived precursors. Such small molecules can spontaneously form nanofiber networks in water through hydrogen bonding, hydrophobic interaction, π–π stacking and electrostatic interaction, and build self-assembled hydrogels of "drugs are materials" [29,30]. They can exert their own pharmacological effects such as anti-inflammatory and antioxidant, demonstrating unique advantages in various oral treatment systems. However, its adhesive stability is greatly affected by the environment, and the repeatability and large-scale preparation of the system still need further optimization.
The formation mechanism of hydrogels is the core basis for the realization of its structure and function. According to the different cross-linking modes, the formation mechanism of oral hydrogels can be divided into four types: physical cross-linking, chemical cross-linking, self-assembly driven and metal ion coordination. Reasonable selection of cross-linking mechanism is helpful to build hydrogel system that can meet specific drug release requirements.
Physical crosslinked hydrogels are three-dimensional network structures spontaneously formed in the water environment through non covalent interactions such as hydrogen bonding, van der Waals force, hydrophobic interaction and electrostatic interaction. This crosslinking method does not require chemical crosslinking agents or initiators, avoiding potential toxic residues, and therefore has higher biological safety and application advantages in oral drug delivery [31]. Li et al. [32] form a strong hydrogen bonding network between −OH on the hemicellulose chain and −COOH and −OH on the oxidized graphene, with oxidized graphene serving as a structural scaffold to stabilize the network (Fig. 2A). Physically crosslinked hydrogels can undergo structural transformation in response to external conditions, enabling targeted drug delivery, and enhancing drug bioavailability and therapeutic efficacy [33,34]. Their simple, safe, and highly controllable preparation process further highlights their potential for treating various diseases and developing oral sustained-release formulations.
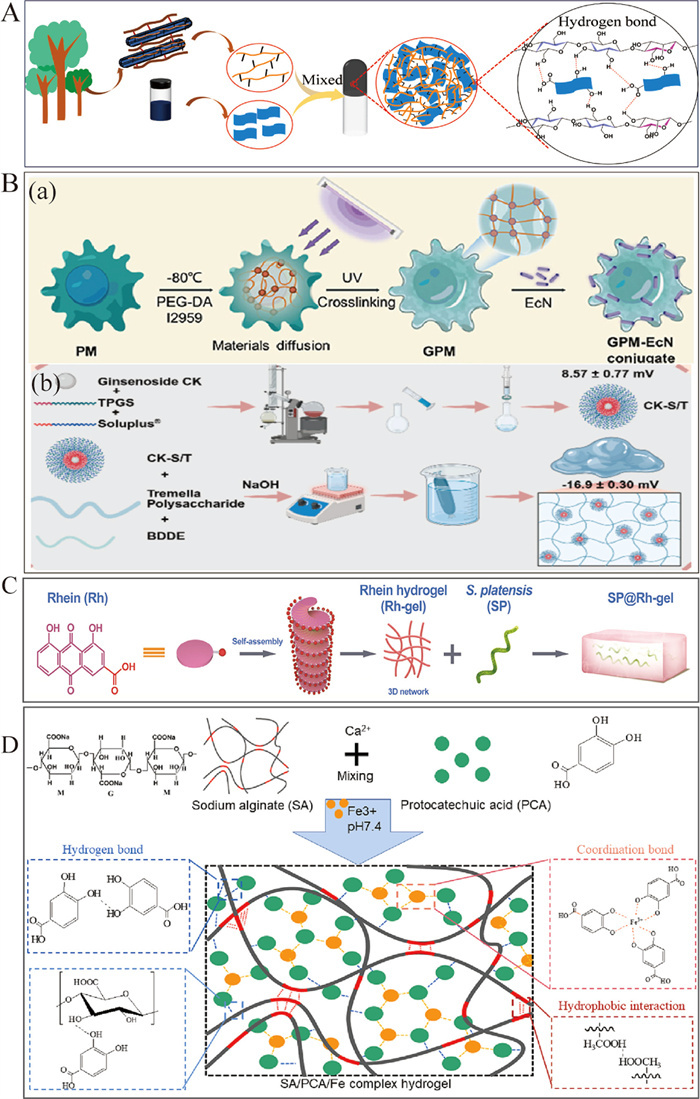
Chemically crosslinked hydrogels are three-dimensional networks constructed by forming permanent covalent bonds between polymer chains. They are usually realized by crosslinking agents, photoinitiation or chemical reactions, and have highly stable and irreversible structural characteristics [35]. In oral hydrogels, the common chemical crosslinking methods include free radical polymerization and amidation reaction. In free radical polymerization, initiators such as potassium persulfate and ammonium persulfate generate free radicals under heat. These free radicals react and bind to the active sites of monomers such as acrylic acid with mountain apricot gum [36], chondroitin sulfate [37], CS [38], and then cross link between molecular chains through the action of cross-linking agent, finally forming a stable copolymer hydrogel network. Amidation reactions involve the formation of amide bonds (–CONH–) between carboxyl (–COOH) and amino groups (–NH2), typically catalyzed by crosslinking agents like ethyldimethylaminopropyl carbodiimide/N-hydroxysuccinimide (EDC/NHS) [39]. Additionally, there are other covalent reactions that can help the formation of hydrogels. Wang et al. [40] chemically crosslinked Tremella fuciformis polysaccharides with 1,4-butanediol diglycidyl ether under alkaline conditions. The epoxy group in 1,4-butanediol diglycidyl ether reacted with −OH on the polysaccharide chain via ring-opening reactions, forming stable ether bonds (C−O−C) to enhance the hydrogel mechanical properties and adhesion. The cross-linking mechanism is shown in Fig. 2B.
Self-assembled hydrogels spontaneously form dynamic, reversible three-dimensional networks via non-covalent interactions. These hydrogels adapt to environmental changes by adjusting their structures and properties, typically using natural biomolecular chemical groups without the need for unnatural functional modifications. During self-assembly, building blocks frequently form high-aspect-ratio structures, which further aggregate into hydrogel networks via physical entanglement or non-covalent binding. Under controlled conditions, small molecules form hydrogels mainly through several non-covalent forces: (1) Hydrogen bonding and hydrophobic interaction. Hu et al. [41] utilized amyloid fibers as templates, onto which polyphenols such as epigallocatechin gallate deposited through hydrogen bonding and hydrophobic interactions. With increasing polyphenol content, hybrid nanofibers formed and aggregated into three-dimensional hydrogels. (2) π-π stacking, involving aromatic groups with conjugated π-electron systems, is another critical driving force in molecular self-assembly. Zhong et al. [42] find that Rhein can form a multi-component crosslinked hydrogels under physiological pH conditions through π-π stacking, hydrogen bonding, and electrostatic interaction, as shown in Fig. 2C. Lu et al. [43] carried out molecular self-assembly through the amphoteric structure of glycyrrhizic acid to form a basic network structure, subsequently strengthened by coordination bonds between Zn2+ ions and carboxyl groups, significantly improving hydrogel stability and mechanical performance. Self-assembled hydrogels, with their dynamic structure and multifunctional design strategy, enable pharmacologically active ingredients to replace inactive carriers. However, they may show excessive swelling or structural disintegration in the GI environment, and their stability and controllability still need to be enhanced through co assembly, ionic modification and other ways.
Certain drugs contain abundant metal coordination groups, such as amino, carboxyl, heterocyclic oxygen, and nitrogen groups, which can coordinate with various metal ions to form hydrogels. Metal ions and organic ligands establish coordination bonds through Lewis acid-base interactions. These bonds, with strengths between weak intermolecular forces and strong covalent bonds, provide dynamic stability in complex environments [44]. Jing et al. [45] successfully constructed a three-dimensional hydrogel network and prepared stable hydrogel beads by coordinating Fe3+ with –COOH and –OH groups in sodium carboxymethyl cellulose and ginger polysaccharide molecules. Zhang et al. [46] further proved that natural polyphenols and organic acids in traditional Chinese medicine are rich in carboxyl and phenolic hydroxyl groups, which can form a coordination structure with Fe3+, and build a stable hydrogel system of traditional Chinese medicine. In addition, natural polyphenolic compounds like proanthocyanidins [17] and protocatechuic acid [47] can form metal-phenol matrix network by non-covalent coordination with metal ions such as Ca2+ and Fe3+ (Fig. 2D). These hydrogels exhibit excellent stability and sustained release characteristics in the GI environment, providing a new strategy for targeted drug release and improving bioavailability.
The intelligent design of oral hydrogels integrates advanced material science with biomedical needs, enabling precise drug release, targeted delivery, and improved bioavailability in response to the dynamic GI environment. This approach addresses limitations of traditional oral formulations, such as drug degradation, low absorption, and poor targeting, while offering excellent biocompatibility and multifunctionality. These innovations provide robust technical support for treating complex diseases and advancing personalized drug delivery systems. Table S1 (Supporting information) [30,48-67] lists the latest research strategies of intelligent hydrogels for oral administration in recent year.
Oral drugs pass through the stomach, duodenum and small intestine in turn, and each part will encounter different pH environments, providing a natural trigger condition for the construction of pH responsiveness of hydrogels. pH responsive hydrogels achieve their functional properties mainly through two mechanisms: one is to induce the formation of hydrogel structure in situ under specific pH conditions. This kind of hydrogel system is designed to realize the liquid gel phase transition, that is, when orally administered, it enters the body in the form of liquid, and forms a three-dimensional gel network under specific pH conditions. This mechanism often depends on the hydrolysis sensitive or conformational reversible nano precursor structure, which releases or exposes the cross-linking site at a specific pH and induces the in-situ formation of hydrogels [48,49,68]. The other type relies on the protonation/deprotonation process of ionizable groups (such as carboxyl and amino groups) in the network structure of the hydrogels, so as to prevent premature drug release and increase the drug concentration of the target (Fig. 3) [69]. In acidic environment, protonation reduces electrostatic repulsion between polymers, shrinks the structure of hydrogels, and limits drug release; In neutral or alkaline environments, deprotonation enhances the negative charge density of the network, increases electrostatic repulsion and hydration ability, triggers swelling, and promotes drug diffusion and release [50-52]. These two mechanisms can be used separately or jointly designed in practical applications, providing an effective strategic basis for achieving targeted and intelligent oral drug delivery.
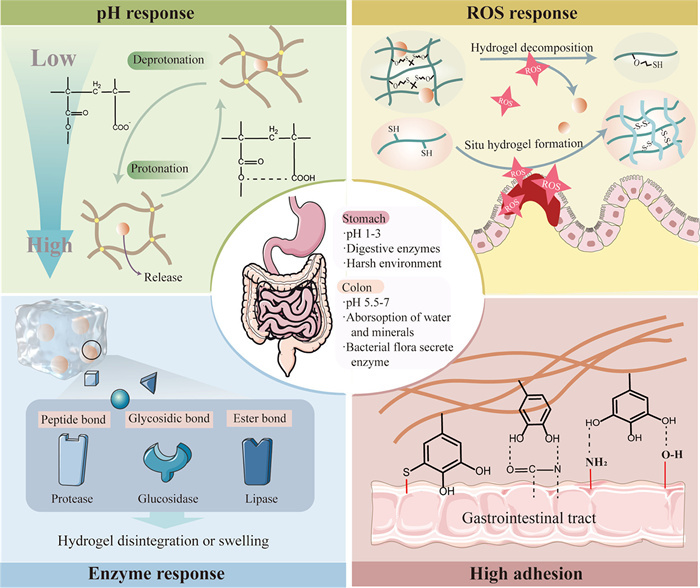
ROS are common microenvironmental features in various lesion areas. The ROS level in pathological state can be dozens of times higher than that in normal tissues, providing a potential target trigger signal for the hydrogel system. Zhang et al. [57] designed a ROS responsive pre-gel system based on mercapto modified hyaluronic acid (HA-SH), which uses the mercapto group to oxidize into disulfide bonds in a highly reactive oxygen environment, thus realizing in situ gel formation. In addition, Huang et al. [58] constructed a ROS responsive hydrogel system formed under physiological conditions. Thione groups introduced in the design can be specifically oxidized by ROS at the inflammatory site, triggering the disintegration of the hydrogels and releasing the encapsulated probiotics. Therefore, ROS responsive hydrogels show great potential to provide more effective solutions for the treatment of inflammatory diseases (Fig. 3).
Enzyme responsive hydrogels are a kind of intelligent delivery system that can change its structure and trigger drug release under specific enzyme mediated conditions (Fig. 3). In the intestinal inflammatory environment, matrix metalloproteinases (MMPs) can specifically recognize and hydrolyze the ester bond of ascorbyl palmitate in the silk fibroin aggregate, trigger the gradual release of Fe3+ and participate in the chelation reaction, at the same time, the quinone group covalently interacts with the amino group on the surface of intestinal epithelium, forming an adhesive hydrogel structure, and enhancing local retention and treatment efficiency [59]. In addition, some colonic enzymes can selectively degrade polysaccharide networks to achieve sustained drug release [30]. In order to improve the targeting and release accuracy, the researchers also constructed the enzyme pH double response hydrogel system. For example, budesonide loaded pectin/polyacrylamide composite hydrogels have stable structure and low swelling under the condition of gastric acid, but it is rapidly degraded in the presence of colonic enzymes, so as to achieve targeted release and reduce systematic side effects [70]. Enzymatic responsive hydrogels represent an intelligent strategy, which uses disease specific enzyme activity for precise drug release and has significant therapeutic potential for GI and systemic diseases. However, the complexity and variability of intestinal microbiota may lead to unpredictable release rate, which highlights the need for more personalized and controllable hydrogel design.
Complex mechanical movements of the GI tract often reduce hydrogel adhesion, resulting in premature hydrogel loss and diminished therapeutic efficacy. Therefore, designing highly adhesive hydrogels is critical for effective in situ treatment of GI diseases. In colonic mucositis, the depletion of the mucosal layer and accumulation of positively charged proteins on damaged epithelial surfaces provide molecular targets for negatively charged adhesive hydrogels. Additionally, chemical modification of hydrogels using adhesive functional groups (e.g., catechol groups) enables covalent and noncovalent binding to nucleophilic sites, such as amides, thiols, and amines, present on tissue surfaces, thereby enhancing retention and improving therapeutic outcomes (Fig. 3) [61]. For instance, hydrogels incorporating ionized N-acrylylphenylalanine and N-[tris(hydroxymethyl)methyl] acrylamide (THMA) exhibit strong gastric tissue adhesion. Under acidic gastric conditions, iAPA transitions from hydrophilic to hydrophobic, promoting hydrogen bond formation assisted by phenyl groups, which exclude surface water and facilitate strong interfacial interactions between THMA and gastric tissue [62]. Similarly, hybrid hydrogels combining gallic acid and SA utilize pyrogallol groups from gallic acid for robust adhesion to intestinal mucosa, achieving over 24-h retention [63]. Alternatively, leveraging the receptor-binding ability of folic acid and hydrogen-bonding properties of protocatechuic acid, hydrogel adhesion to intestinal mucosa is significantly enhanced, maintaining localization at inflammation sites for up to 6 h [71]. In summary, developing strongly adhesive hydrogels effectively addresses challenges posed by GI tract movements, reinforces interactions with damaged mucosa, and substantially improves therapeutic performance. Nevertheless, excessive adhesion must be carefully managed, as overly strong interactions may lead to undesirable residues, or compromise hydrogel flexibility.
Oral hydrogels need to overcome harsh conditions of the digestive tract and the shear stress of GI peristalsis, resulting in rupture or deformation. The self-healing property can quickly repair damage, preserving its structural integrity and mechanical strength, preventing premature drug release, and enhancing delivery reliability [72]. For instance, a self-healing hydrogels designed for oral probiotic protection, synthesized via a sulfhydryl-Michael addition reaction, exhibits rapid self-repair, porous structure, mechanical robustness, and responsiveness to GI conditions (Fig. 4A) [65]. Such self-healing characteristics ensure hydrogels effectively resist mechanical stress inherent in GI peristalsis, maintaining their structural integrity and protecting encapsulated therapeutics. However, the development of self-healing hydrogels still faces challenges, including balancing rapid healing capability with practical preparation methods and costs. Future research should prioritize improving self-healing efficiency and affordability to ensure wider clinical applicability.
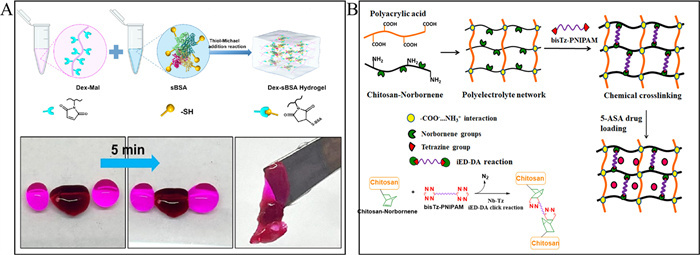
The GI tract maintains a stable temperature of approximately 37 ℃, which can be leveraged by thermally responsive hydrogels to enhance drug delivery. These hydrogels encapsulate drugs at lower temperatures in vitro and release them more effectively at body temperature through temperature-responsive mechanisms. Current research often combines temperature and pH responsiveness to develop dual-responsive oral hydrogels, enabling better adaptation to the complex GI environment and enhancing colon-targeted drug delivery. For example, researchers used poly(N-isopropylacrylamide) as a temperature-sensitive monomer and crosslinked with other materials to form a hydrogel for delivering tetracycline [66] and 5-aminosalicylic acid [67] and similar drugs. These hydrogels exhibit optimal drug release efficiency at 37 ℃ and in an alkaline environment, making them ideal carriers for controlled, colon-targeted drug delivery (Fig. 4B). Despite their advantages, the clinical translation of temperature-responsive oral hydrogels faces potential challenges, such as precise tuning of transition temperatures, biocompatibility, and stability under variable in vivo conditions. Future research should address these issues to maximize therapeutic efficacy and safety.
As a drug delivery platform, the drug loading mode of hydrogels directly determines the stability, release characteristics and treatment efficiency of the system. According to the interaction mode between drugs and gel network, the drug loading mechanism of oral hydrogel system mainly includes physical embedding, covalent conjugation and composite delivery structure.
Physical embedding is the most common way of drug loading in hydrogels. Drug molecules are fixed in the gel network or its pore structure through non covalent interactions. This method has mild preparation conditions and is suitable for encapsulating temperature sensitive or easily degradable drugs. It is widely used as a drug carrier for oral small molecules [73,74]. However, this method usually has limited loading efficiency and initial burst release phenomenon, making it difficult to achieve precise regulation of release rate, especially in complex GI environments where stability is relatively poor.
The covalent binding drug delivery strategy combines drugs with hydrogel matrix through chemical bonds, which helps to improve the structural stability of hydrogel drug delivery and achieve environmentally responsive release. For example, Fraile-Gutierrez et al. [75] first form enzyme crosslinking agent covalent complexes by azide alkyne click reaction of modified β-galactosidase, and then crosslink with azide CS to form a hydrogel network, achieving embedded covalent immobilization of enzymes, effectively protecting enzyme activity in GI environment and improving delivery stability. However, this strategy requires high demands on the molecular structure of the drug, and may lead to partial inactivation or conformational changes of some bioactive substances during covalent reactions. Its application in oral formulations still faces conversion barriers.
Recently, the application scope of oral hydrogels has expanded from drug release systems to more sophisticated micro/nanostructured carriers. The composite delivery system usually adopts a "multi-layer structure" design, which first encapsulates drugs in primary carriers such as microspheres, nanoparticles, liposomes or micelles, and then further embeds them into the hydrogel network to form a composite structure [76,77]. This method can give consideration to the biological protection ability of nano delivery system and the controlled release characteristics of hydrogels. The composite system can enhance oral stability, improve bioavailability, and achieve multi-mode release regulation. However, its preparation process is complex, involving multiple steps of drug loading, encapsulation, and gelation, which may result in a lower total drug loading capacity, and there are still certain challenges in the large-scale production of the system.
Hydrogel systems, with their unique physical and chemical properties, offer innovative solutions for oral drug delivery. These systems enable sustained release, targeted delivery, and intelligent drug response, significantly enhancing bioavailability while minimizing rapid degradation and side effects in vivo. In this section, we focus on the latest research progress of oral hydrogels in different diseases, showing their good potential for clinical application.
The esophagus is a tube that connects the mouth with the stomach and is responsible for transporting food and fluids from the throat to the stomach. Due to its insidious early symptoms and poor prognosis in advanced stages, the effective management of precancerous lesions and treatment of esophageal cancer holds significant clinical value. Chronic inflammatory gastroesophageal reflux alters the esophageal microenvironment and induces epithelial metaplasia, a precancerous lesion. Naranjo et al. [80] developed an extracellular matrix (eECM) pre-gel solution derived from acellular porcine esophageal mucosa, which was orally administered to experimental dogs. Upon administration, the eECM hydrogels adhered effectively to the esophageal mucosa under laminar flow conditions and maintained retention for at least 24 h. This system alleviated esophageal inflammation, modulating local immune responses, suppressed TNF-α expression, and in some cases reversed metaplasia and restored normal squamous epithelium. Gong et al. [81] developed a thermosensitive hydrogel composed of F127 and tannic acid for in situ drug delivery of esophageal cancer. The system achieved continuous fluorescence signal retention for up to 24 h in the mouse esophagus, and continued to release capsule drugs used to treat esophageal cancer by restoring p53 activity and enhancing T cell immunity, showing its excellent delivery stability and biological performance. In summary, oral hydrogel systems offer innovative strategies for treating esophageal diseases by improving precancerous lesions, reducing inflammation, and enhancing therapeutic outcomes in esophageal cancer.
Gastric diseases are common worldwide, including gastric ulcers, gastritis, and Helicobacter pylori (H. pylori) infection. In recent years, hydrogels have been widely studied as gastric retention systems due to their unique physical and chemical properties [87]. These hydrogels maintain stability in acidic gastric environments, enhance drug adhesion, and extend therapeutic efficacy by regulating drug release rates.
H. pylori infection is a primary cause of gastritis, gastric ulcers, and gastric cancer. Traditional antibiotic therapies require prolonged administration, but their effectiveness is often compromised by drug degradation in acidic gastric environments. Oral hydrogel delivery systems address these limitations by protecting drugs from degradation, enhancing localized drug concentrations, prolonging release, and potentially reducing antibiotic resistance. For instance, porous hydrogels incorporating guar gum exhibit gastric adhesiveness and buoyancy, maintaining mechanical stability and effectively sustaining amoxicillin release under varying gastric pH conditions [78]. Similarly, a crosslinked SA-carboxymethyl cellulose hydrogels successfully encapsulated furazolidone (71%–76% efficiency) and bismuth (Ⅲ) ions (88% efficiency), exhibiting significant swelling and prolonged stability in gastric fluids. This formulation demonstrated controlled drug release and substantial anti-H. pylori activity [79]. Additionally, antibacterial peptide hydrogels rapidly release antimicrobial peptides in acidic environments, effectively eliminating H. pylori without proton pump inhibitors, representing a promising antibiotic-free therapeutic alternative [80]. Beyond drug encapsulation, multifunctional oral hydrogels offer targeted and synergistic strategies against H. pylori. For example, a pH-responsive metal-organic framework hydrogen production nanoparticle effectively targets inflamed gastric tissue via electrostatic interactions. Upon gastric hydrolysis, it releases Zn2+ and H2, simultaneously eradicating bacteria and repairing gastric mucosal damage [81]. Similarly, CS hydrogels functionalized with benzophenone tetracarboxyimide benzoyl thiourea selectively inhibit cyclooxygenase-2, providing targeted anti-inflammatory effects against infection-related inflammation [82]. Another innovative antibiotic-free approach utilizes a multifunctional organic copper framework within ascorbyl palmitate hydrogels to target infection sites, disrupt H. pylori biofilms, and eliminate intracellular bacteria, showing significant therapeutic promise [83]. In summary, oral hydrogels offer innovative, multifunctional platforms for effectively treating H. pylori infection. However, future clinical translation will require addressing key challenges, including ensuring biocompatibility, long-term stability, precise drug release control, and balancing therapeutic efficacy with patient safety.
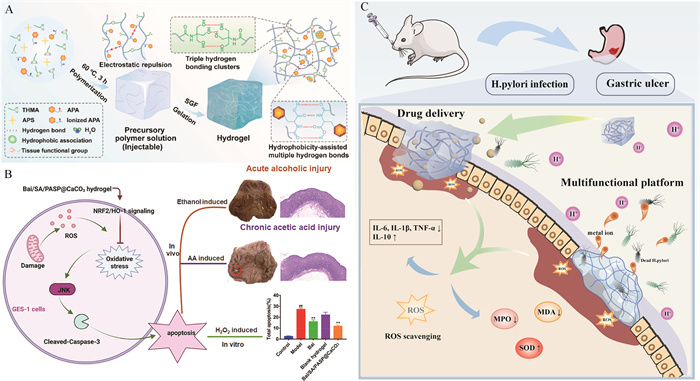
Gastric ulcers, a common digestive disorder, involve damage to the gastric mucosa, often leading to painful lesions. Oral hydrogels offer substantial therapeutic benefits for treating gastric ulcers. By forming an adhesive barrier at the ulcer site, they protect the gastric wall from further damage caused by gastric acid and pepsin, effectively alleviating pain. For example, a high-viscosity keratin hydrogel showed excellent gastric retention (up to 12 h) and effective mucosal adhesion, significantly promoting healing in ethanol-induced gastric ulcer models [84]. Xie et al. [62] developed a novel bioadhesive hydrogel that forms in situ and provides firm adhesion to gastric tissue, effectively protecting wounds from gastric acid and pepsin damage (Fig. 5A). Another innovative hydrogels utilizing thiourea-catechol reaction demonstrated prolonged adhesion (> 48 h), rapid gelation under acidic conditions, effective hemostasis, anti-inflammatory effects, and accelerated healing by promoting growth factor accumulation, cellular proliferation, and vascular regeneration [61]. Beyond as protective barriers, hydrogels can serve as drug delivery platforms to accelerate ulcer healing [85]. Xu et al. [86] designed a SA/polyaspartic acid/CaCO3 in-situ hydrogels loaded with baicalin. These hydrogels continuously release baicalin in the gastric intima (only 15% in 2 h and 49% in 7 h), increasing the protein levels of NRF2, HO-1, and Bcl2, while reducing p-JNK, cleaved-caspase-3, and Bax lever, thus alleviating acute and chronic gastric ulcers (Fig. 5B). Therefore, oral hydrogels provide a multifaceted approach to gastric ulcer treatment, combining precise drug delivery, sustained adhesive protection, and enhanced mucosal healing. These features offer a safer and more effective treatment option, presenting significant potential for clinical application (Fig. 5C).
The intestine is an important component of the human digestive system, involving multiple key functions such as nutrient absorption and immune regulation. However, the incidence of intestinal diseases is increasing year by year, including inflammatory bowel disease (IBD), irritable bowel syndrome, intestinal infection, and colorectal cancer. Traditional treatment methods such as oral medication and local treatment often limit their efficacy due to poor stability, insufficient absorption, and significant side effects of the drugs in the intestine. In contrast, oral hydrogels have shown great potential in the treatment of intestinal diseases due to their excellent biocompatibility, adhesion, and drug-release ability. By targeting drug delivery and providing sustained pharmacodynamic effects, hydrogels are expected to significantly improve the treatment experience of patients and improve the treatment effect.
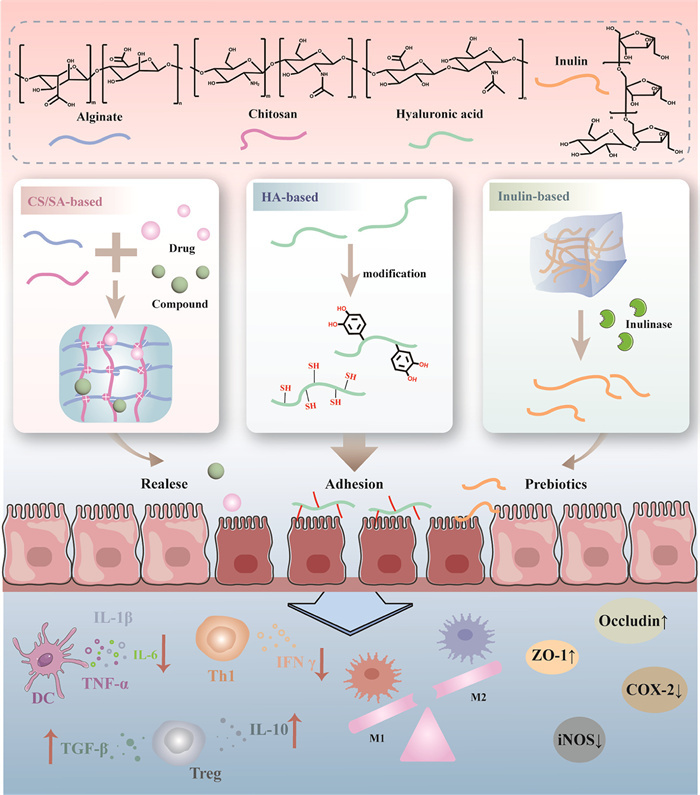
IBD includes Crohn's disease (CD) and ulcerative colitis (UC), characterized by chronic intestinal inflammation, immune imbalance, and disrupted gut microbiota. Due to the frequent occurrence of intestinal barrier damage and recurrent inflammatory reactions in IBD patients, drug delivery systems face challenges such as GI barrier, poor targeting, and low bioavailability. In recent years, oral hydrogels based on natural polymers have shown great potential in the treatment of IBD. Such systems typically have the following common mechanisms: they can act as probiotic carriers to regulate gut microbiota, deliver anti-inflammatory drugs in a sustained manner, enhance local adhesion in the intestine to prolong retention time, and to some extent promote epithelial repair and protect active ingredients from GI environmental damage. On this basis, different types of natural polymer materials exhibit unique advantages in structural design, gelation behavior, and drug delivery function due to their differences in physicochemical properties. The following sections will introduce the specific applications and performance differences of several representative hydrogel materials in the treatment of IBD (Fig. 6).
(1) Alginate-based hydrogels
SA, a natural polysaccharide containing carboxyl groups, has excellent pH responsiveness and gelling ability, and is widely used to construct oral hydrogels to cope with gastric acid environment and achieve colon release. SA based hydrogels can be loaded with a variety of therapeutic factors, including siRNA@MOF Nanoparticles are used to target inflammatory macrophages and accumulate in the colon, effectively alleviating UC [87], In addition, SA microspheres loaded with bioactive glass [88] or M2 macrophage membrane-coated Janus nanomotor [89] exhibit enhanced ROS clearance and tissue repair capabilities. SA can also be combined with probiotics to synergistically regulate gut microbiota and enhance therapeutic efficacy through its protective structure [90].
(2) Chitosan-based hydrogels
CS is a positively charged natural polysaccharide with good biological adhesion and film-forming properties. The electrostatic interaction between it and alginate can form stable CS/SA hydrogels at low pH, which can be used to protect drugs in oral delivery systems and achieve colon targeting. This type of hydrogels has been used to deliver a variety of functional nanostructures, such as Pluronic F127 modified gold nanoparticles [91] and silk fibroin-based nanoparticle with the surface functionalization of antimicrobial peptides [92], which can alleviate intestinal oxidative stress, promote epithelial repair and macrophage polarization. In addition, CS/SA hydrogels can also be used as exosome carrier to protect its activity in the intestine and achieve targeted release [20].
(3) Hyaluronic acid-based hydrogels
HA is an anionic glycosaminoglycan with natural anti-inflammatory and adhesive properties. Although it does not have the ability of self-gelling, it can achieve intelligent response and in-situ gelling through chemical modification, and is suitable for constructing oral hydrogels to deal with inflammation microenvironment. The HA based ROS reactive hydrogels can selectively respond to the inflammatory colon region and locally release encapsulated probiotics (such as Lactobacillus reuteri) to alleviate inflammation [58]. In addition, HA modified with dopamine (DA) has excellent self-adhesive and self-healing properties, and can form adhesive in situ at the lesion site, enhancing retention and therapeutic effect [93]. Self crosslinked HA-DA hydrogels significantly enhanced colon adhesion, and the adhesion strength was 3.81 times higher than that of HA. And demonstrated excellent inflammation relief and barrier repair abilities in animal models.
(4) Inulin based hydrogels
Inulin is a natural prebiotic that can be specifically degraded by colonic microbiota and has unique advantages in regulating gut microbiota [94]. The hydrogels based on inulin can load a variety of drugs, such as nano enzyme complex and anti-fibrosis drug pirfenidone, to achieve long-term GI stay and targeted delivery at the colon [95]. These systems can effectively alleviate IBD symptoms by inhibiting inflammatory pathways such as transforming growth factor-β (TGF-β)/Smad, clearing ROS, and improving intestinal epithelial barrier function. In addition, inulin hydrogels have good bioadhesiveness, which helps to increase local drug concentration and reduce disease recurrence rate [30].
In summary, oral hydrogels based on SA, CS, HA, and inulin offer advanced multifunctional platforms for targeted GI drug delivery. By providing protective encapsulation, controlled release, and enhanced bioadhesion, these hydrogels represent promising strategies to effectively treat gastrointestinal diseases, promote mucosal healing, and restore microbial balance. Nonetheless, future research should focus on optimizing release kinetics, bioadhesion strength, and clinical safety profiles to facilitate their translation into practical therapeutic applications.
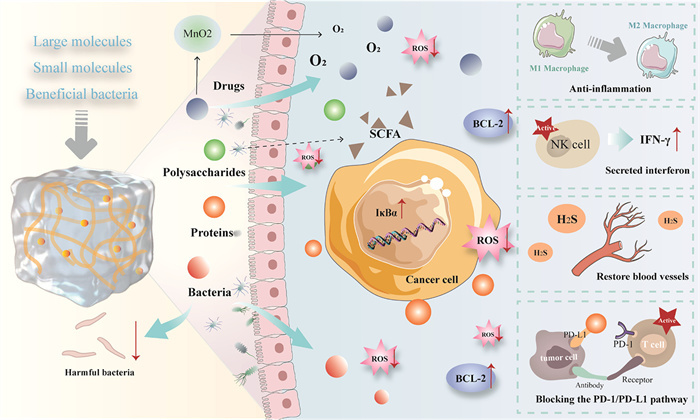
Colon cancer is one of the most common malignant tumors of the digestive tract. Traditional chemotherapy drugs are highly toxic and difficult to maintain sufficient drug concentrations at the tumor site. Oral hydrogels have emerged as promising drug carriers due to their excellent biocompatibility, targeted delivery capabilities, and controlled degradation profiles, enabling efficient encapsulation and precise release of small molecule drugs, macromolecular polysaccharides, proteins, and probiotics (Fig. 7).
(1) Delivery of macromolecular polysaccharides and proteins
Macromolecular polysaccharides and proteins are promising candidates for incorporation into oral hydrogel systems due to their potential in immune regulation and biological activity, which can inhibit tumor growth by modulating the immune microenvironment and reducing inflammation [96]. Li et al. [97] developed a water-soluble CS hydrogel loaded with the protein hydrolysis-resistant d-peptide oral programmed cell death ligand 1 (PD-L1) binding peptide 1 (OPBP-1). This formulation increased oral bioavailability to 52.8% and extended its half-life to 14.55 h, effectively blocking the PD-1/PD-L1 interaction and enhancing interferon-γ (IFN-γ) secretion from CD8+ T cells, thereby significantly inhibiting tumor growth. El Deeb et al. [98] encapsulated a polysaccharide extracted from white mushrooms into SA/κ-carrageenan hydrogel microcapsules, which activated intestinal NK cells, promoted anti-tumor immune responses, and induced apoptosis in cancer cells, offering potential resistance against colon cancer.
(2) Delivery of small molecule drugs
Oral hydrogels enable precise, controlled release of chemotherapeutics and small-molecule drugs derived from traditional medicine, concentrating drug action at tumor sites while minimizing systemic toxicity [99,100]. For instance, a hydrogel system embedding hollow manganese dioxide nanocarriers loaded with oxaliplatin (drug loading capacity 45.0 wt%) adhered effectively to colon tumors, activating anti-tumor immune pathways (HDACs/ID2/IL-12 receptor) and significantly enhancing therapeutic outcomes [101]. Similarly, porous manganese oxide-based nanomotors, encapsulated within CS/SA alginate hydrogels, enabled efficient mucosal traversal and tumor penetration. It achieved multi-responsive drug release, reversed immunosuppression, induced tumor cell death, and effectively inhibited both primary and distant tumors [102]. Additionally, the intelligent hydroxypropyl-β-cyclodextrin polymer networks used for cytarabine delivery showed an extended drug plasma half-life (8.75 h) and bioavailability, indicating strong potential for colon cancer therapy [103]. Hydrogels prepared from natural naringenin-soy protein complexes notably improved drug solubility and exhibited sustained drug release, enhancing cytotoxicity against colorectal cancer cells [104]. These examples highlight the versatility and promise of hydrogel-based drug delivery in colon cancer treatment.
(3) Deliver probiotics
In recent years, embedding bacteria within hydrogel systems has garnered significant attention. Hydrogels can protect probiotics, facilitate their colonization in the intestine, regulate the tumor microenvironment, and enhance host immunity through microbial metabolites. Li et al. [105] reported the development of a thiolated HA hydrogel loaded with Thiobacillus denitrificans, creating a bacterial hydrogel for targeted colon adhesion. This system effectively removes excess H2S in colon cancer, normalizes tumor blood vessels, and improves the delivery of chemotherapy drug camptothecin, thereby inhibiting tumor progression. Zhu et al. [106] designed a probiotic Enterococcus faecium strain encapsulated in HA-inulin for targeted colon delivery. This approach targets Clostridium perfringens, reducing its abundance in the colon, slowing tumor growth, improving the tumor microenvironment, and enhancing anti-cancer treatment efficacy. Thus, oral hydrogels offer a promising strategy for safer and more effective colon cancer treatment by improving drug retention at the tumor site, reducing systemic toxicity, and boosting therapeutic outcomes.
The prevalence of obesity has almost doubled in the past 40 years. Oral hydrogels can expand in the stomach by absorbing water, occupying volume, and creating a sense of satiety. It can also be used to help control appetite and intake to reduce weight and control obesity. Madaghiele et al. [107] developed a cellulose-based superabsorbent hydrogel that absorbs water, increases volume in the gastrointestinal tract, and reduces the energy density of food. These hydrogels remain undigested through the stomach and small intestine, rehydrate in the colon, and are partially enzymatically degraded before excretion. Silvestri et al. [108] discussed a biomimetic superabsorbent hydrogel that can prevent obesity and metabolic syndrome by protecting the intestinal barrier and improving the gut microbiota composition. Le et al. [109] introduced a double-network hydrogel with 100 times the mechanical strength and double the swelling capacity of the original single-network hydrogels. These hydrogels maintain volume and elasticity in the digestive system without increasing heat, prolongs satiety, and reduces energy density (Fig. S1A in Supporting information). These innovations offer potential solutions for weight loss and obesity management.
Diabetes is a hyperglycemic condition that increases the risk of serious complications. Insulin is the most effective treatment, but its oral delivery faces significant challenges due to the acidic environment of the gastrointestinal tract and enzymatic degradation, which can inactivate insulin and reduce its bioavailability. Oral hydrogels have been widely used to protect insulin and ensure its controlled release at the appropriate site and time. Hydrogel-encapsulated insulin offers good loading efficiency [51,110], and continuous hypoglycemic effect [111,112]. Ren et al. [113] developed an oral insulin delivery strategy using Chlorella vulgaris and SA, which involves two mechanisms of insulin absorption: direct release from the hydrogels and endocytosis by M cells and macrophages. This system provides a more effective and lasting hypoglycemic effect than insulin injection, without causing intestinal damage (Fig. S1B in Supporting information). Additionally, glucose-responsive hydrogels, designed using phenylboronic acid or glucose oxidase-mediated crosslinking, can detect blood glucose fluctuations and trigger insulin release accordingly, ensuring precise glycemic control [114]. Other research encapsulates Exendin-4 using combined capsules, hydrogel coating, and metal-organic framework nanoparticles, leading to a significant increase in plasma Exendin-4 levels and enhanced endogenous insulin secretion [115]. These approaches hold great promise for the routine treatment of diabetes.
As aging progresses, the proliferative and differentiative capacity of pluripotent stem cells in bone marrow stromal cells diminishes. This, coupled with reduced osteoblast function and increased apoptosis of mature osteoblasts, leads to insufficient bone matrix formation, a key factor in osteoporosis. Recently, the gut-bone axis has emerged as a biological link between the intestines and bones, gaining attention as a potential therapeutic target for osteoporosis. This axis involves various mechanisms, including nutrient absorption, endocrine regulation, and immune signaling, to facilitate bone-intestinal interactions. Qu et al. [116] developed an oral hydrogel microsphere system designed to deliver drugs precisely to bone marrow mesenchymal stem cells via the gut-bone axis. The system extends drug activity, promotes osteogenic differentiation, activates the adenosine 5′-monophosphate (AMP)-activated protein kinase (AMPK)-silent information regulator 1 (SIRT1) pathway, reverses mitochondrial aging in bone marrow mesenchymal stem cells, and fosters bone tissue regeneration. This approach offers a promising strategy for regulating mitochondrial function and preventing bone loss, particularly in the treatment of osteoporosis (Fig. S1C in Supporting information). Similarly, encapsulation of Clostridium sporogenes within oral hydrogels targeted intestinal colonization (staying in the colon area for more than 12 h), thereby enhancing microbiota-driven immune modulation. This approach significantly promoted bone regeneration by utilizing microbiota-derived metabolites and restoring mitochondrial activity within bone marrow derived macrophages (BMMs). Compared with traditional microbiota transplantation, the system only requires 5 doses to achieve the same bone protection effect, with higher compliance and sustainability [117]. Additionally, pH responsive core-shell hydrogel microspheres have been developed to effectively wrap bone targeted nanoparticles to activate the hypoxia-inducible factor-1α (HIF-1α)/vascular endothelial growth factor (VEGF) signaling pathway, inhibiting osteoclast gene expression, reducing bone resorption, enhancing intra-bone vascularization, and slowing postmenopausal osteoporosis progression [118]. In conclusion, oral hydrogel systems represent a promising therapeutic strategy for osteoporosis. Future research should focus on optimizing targeted delivery, prolonging therapeutic efficacy, and evaluating long-term safety to ensure successful clinical translation.
Recent studies have highlighted the detoxification potential of oral hydrogels due to their inherent properties and drug delivery capabilities. For instance, an iron-anchored amyloid hydrogel has been developed as a catalytic platform for alcohol detoxification. These hydrogels exhibit strong catalytic oxidation capacity, rapidly reducing blood alcohol levels and mitigating the risk of acetaldehyde accumulation. Unlike traditional alcohol metabolism, the oral administration of these hydrogels shifts the detoxification process to the gastrointestinal tract, easing the liver's workload. Remarkably, this method does not induce additional gastrointestinal discomfort and significantly alleviates alcohol-induced intestinal damage and microbial imbalance, supporting its potential for clinical application (Fig. S1D in Supporting information) [119]. Oral hydrogels can also address lead poisoning. By encapsulating chlorella and the anti-inflammatory agent berberine, the hydrogels facilitate lead removal from the liver, kidneys, and bones through chelation, antioxidant effects, and modulation of the gut microbiota. It also reduces oxidative stress and tissue damage caused by lead exposure, restores the intestinal barrier, and maintains intestinal microecological balance, offering multiple therapeutic benefits [120]. These systems are biodegradable, cost-effective, and exhibit high biological safety, making them promising candidates for clinical use.
Oral hydrogels hold significant potential for providing efficient, safe, and convenient treatments for cardiovascular and cerebrovascular health, owing to their targeted delivery and sustained drug release properties. Hanafy et al. [121] developed starch-based hydrogels encapsulating anthocyanins to enhance their retention in heart tissue and protect them from lymphatic and immune system clearance. Their studies demonstrated that this system effectively reduces oxidative damage in fibrotic myocardium and liver tissue induced by carbon tetrachloride, restores glycogen levels, and improves histological function, highlighting its potential in treating cardiomyopathy. Sagar et al. [122] prepared SA-starch hydrogel microspheres co-loaded with iron (iron dextran) and anti-inflammatory probiotics (Bifidobacterium brevis). This formulation improved the bioavailability of iron, aiding in the treatment of iron deficiency anemia and reducing associated intestinal inflammation (Fig. S1E in Supporting information). Liu et al. [123] developed an intestinal-targeted "microsphere liposome" composite carrier, which enhanced the delivery, stability, and absorption of astaxanthin by targeting the FcRn receptor on intestinal epithelial cells, offering protection against hypercholesterolemia and cardiovascular risk. Overall, oral hydrogels present considerable promise in advancing cardiovascular health treatments, offering new directions for developing more efficient and safer therapeutic strategies.
Oral hydrogels have been developed for a wide range of innovative applications, enhancing their adaptability in treating various diseases and maximizing their therapeutic potential. Zheng et al. [124] designed a seed hydrogel to eliminate harmful metabolites in liver failure by encapsulating the cascade reaction triggered by Bacillus subtilis and Clostridium butyricum, thereby alleviating liver failure. Wu et al. [125] demonstrated that quercetin nanoparticles loaded into hydrogel microspheres can protect the intestinal barrier, regulate gut microbiota, and alleviate sleep disorders and inflammation induced by high-altitude environments. Han et al. [126] utilized inulin hydrogels to load allergens, significantly prolonging allergen retention in the small intestine. This approach enhances antigen uptake by dendritic cells, modulates intestinal microbiota and metabolites, inhibits pathological Th2 immune responses, and induces regulatory T cells and anti-inflammatory factors, thereby achieving immune tolerance and long-term protection against food allergies. Oral hydrogels also enable the delivery of radiation-protective agents such as amifostine, which reduces hematopoietic system damage in mice caused by γ-radiation and improves survival rates [127]. The pig interferon α/γ also used for delivering fusion can effectively inhibit pseudo rabies virus replication, reduce viral load in tissues, alleviate clinical symptoms and tissue damage caused by infection, and significantly enhance immune response to treat pseudo rabies virus infection [128]. Another innovative approach involves an oral-targeted explosive hydrogel microsphere that activates uric acid transporters, promoting intestinal uric acid excretion, reducing serum uric acid levels, and optimizing gut microbiota structure [129]. These advancements underscore the potential of oral hydrogels in offering non-invasive, effective treatments for a range of conditions.
Oral hydrogels hold significant promise in the treatment of gastrointestinal diseases due to their unique three-dimensional network structure, which enables them to serve as drug carriers with sustained, targeted, and responsive release functions. These hydrogels not only improve drug bioavailability but also minimize side effects on healthy tissues. As research advances, various smart hydrogels have been developed for disease treatment. These hydrogels degrade or respond to specific environmental conditions in the colon, enhancing drug release at targeted sites, and thereby improving treatment efficacy and patient compliance. In addition, combined with a variety of nanomaterials and composite systems, hydrogel systems can better adapt to the complex in vivo environment and play an important role in inflammation regulation, tissue repair, and immune regulation.
With the continuous development of drug delivery technology, hydrogels, as a promising drug-loading material, have been widely used in wound dressings [130], ophthalmic applications [131], tissue engineering [132], and other fields. However, there are still few hydrogels in the field of oral application, and their clinical application still faces multiple challenges. (1) The drug carrying capacity is limited. Because the internal pore structure of the gel has physical restrictions on the drug loading capacity, most hydrogels diffuse into the network through the drug in the water environment. For protein, polypeptide, nucleic acid drugs with large molecular weight, it may be difficult to freely penetrate into the hydrogel structure, resulting in low loading efficiency. (2) The controllability of release is limited. The classification of oral intelligent response hydrogels is still relatively limited, most of which are still pH responsive. When diseases occur, the pH value of the digestive system will change with other pathological characteristics, so the design of hydrogels that can respond to disease characteristics and have multiple reaction mechanisms deserves further research. (3) Difficult to industrialize. Some high-performance hydrogel systems depend on fine conditions and are not suitable for large-scale preparation. Therefore, improving the drug loading performance of hydrogels to meet the needs of complex drug delivery is still the focus of future research.
Oral hydrogels show significant advantages in the treatment of gastrointestinal diseases. They can protect drugs in the harsh gastric environment, enable site-specific release in the gastrointestinal tract, and interact with local tissues or microbiota, making them ideal carriers for treating diseases localized in the GI tract or metabolically regulated. At the same time, with the development of materials and drug loading technology, the application of oral hydrogels has expanded to non-abdominal systemic diseases, such as metabolic diseases, osteoporosis, cardiovascular diseases, etc. The treatment of such diseases often relies on systemic pharmacological effects. Oral hydrogels improve the effect of systematic administration by controlling drug release rate, enhancing bioavailability and protecting drug activity. For example, based on the mechanism of targeted release in specific areas of the intestine, pathways such as gut brain, gut bone, and gut immune axis can be regulated, indirectly improving metabolic or skeletal status. Therefore, the therapeutic effect of hydrogel is not only limited to local effects, but also can realize the potential of systemic treatment through "the intestine as the central node", providing a new treatment strategy for multi system diseases. On the one hand, the development of oral hydrogels in the future can develop more stable, controllable, and intelligently responsive hydrogel materials through the innovation of nanotechnology and materials science, so that they can achieve precise release under different disease characteristics or environmental responses. On the other hand, by combining hydrogels with other novel drug delivery systems, more versatile composite hydrogels can be developed. These composite hydrogels can not only carry multiple drugs, but also achieve multiple functions during release, enabling more comprehensive disease management. Small molecule self-assembled hydrogels have attracted extensive attention due to their advantages of convenient operation, large drug loading, and no introduction of additional compounds. At present, relevant research has involved multiple application fields such as neuroinflammation [133] and traumatic brain injury [134]. However, compared with the study of self-assembly to form nanoparticles, the exploration of self-assembly of small molecules to form hydrogels is still insufficient, especially in the field of oral application. Therefore, it is a worthy research direction to explore the self-assembly of small molecular compounds such as traditional Chinese medicine components to form hydrogels and combine their pharmacodynamic effects for the treatment of multi-system diseases. With the advancement of technology and interdisciplinary collaboration, oral hydrogels are expected to play an important role in the personalized treatment and targeted therapy of gastrointestinal diseases, providing patients with a better treatment experience.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Peishuang Yu: Writing – review & editing, Writing – original draft, Validation. Bohan Chen: Writing – review & editing, Visualization. Bingyu Xie: Investigation, Data curation. Mengjiao Zhou: Resources, Methodology. Chengying Wang: Investigation, Data curation. Shenshen Yang: Writing – original draft, Supervision. Wei Huang: Writing – review & editing, Conceptualization. Yubo Li: Supervision, Conceptualization.
This work was supported by the National Natural Science Foundation of China (Nos. 82374300, 82474217) and CAMS Innovation Fund for Medical Sciences (CIFMS) (No. 2021-I2M-1-026).
Supplementary material associated with this article can be found, in the online version, at doi:
X. Luo, E.L.S. Fong, C. Zhu, et al., Acta Biomater. 132 (2021) 461–472. doi: 10.1016/j.actbio.2020.12.037
Y. Wei, X. Zhou, Z. Li, et al., Adv. Sci. 12 (2025) e2405054. doi: 10.1002/advs.202405054
Y. Liang, S. Li, Y. Pan, et al., Chin. Chem. Lett. 36 (2025) 110841. doi: 10.1016/j.cclet.2025.110841
G.W. Liu, M.J. Pickett, J.L.P. Kuosmanen, et al., Nat. Mater. 23 (2024) 1292–1299. doi: 10.1038/s41563-024-01811-5
Y. Cao, K. Cheng, M. Yang, et al., J. Nanobiotechnology 21 (2023) 21. doi: 10.1186/s12951-023-01770-0
M. Ren, N. Li, X. Jiang, et al., Colloids Surfaces B: Biointerfaces 220 (2022) 112862. doi: 10.1016/j.colsurfb.2022.112862
S. Aghlara-Fotovat, E. Musteata, M.D. Doerfert, et al., Biomaterials 301 (2023) 122246. doi: 10.1016/j.biomaterials.2023.122246
W. Ji, P. Zhang, Y. Zhou, et al., J. Control. Release 367 (2024) 93–106. doi: 10.1016/j.jconrel.2024.01.014
C. Wang, H. Tang, Y. Duan, et al., J. Colloid Interface Sci. 674 (2024) 92–107. doi: 10.1016/j.jcis.2024.06.102
I. Usach, R. Martinez, T. Festini, J.E. Peris, Adv. Ther. 36 (2019) 2986–2996. doi: 10.1007/s12325-019-01101-6
S.K. Agrawal, P. Kumari, Biosystems, Biomed. Drug Deliv. Systems (2024) 43–59. doi: 10.1007/978-981-97-2596-0_3
J. Shangguan, F. Yu, B. Ding, et al., Acta Biomater. 184 (2024) 127–143. doi: 10.1016/j.actbio.2024.06.021
S. Hua, Front. Pharmacol. 11 (2020) 524. doi: 10.3389/fphar.2020.00524
Y. Xu, N. Shrestha, V. Preat, A. Beloqui, J. Control. Release 322 (2020) 486–508. doi: 10.1016/j.jconrel.2020.04.006
F. Deng, Y.H. Bae, J. Control. Release 327 (2020) 100–116. doi: 10.1016/j.jconrel.2020.07.034
B. Li, X. Li, X. Chu, et al., Bioact. Mater. 15 (2022) 305–315.
Y. Zhang, Y. Wang, X. Zhang, et al., ACS Nano 18 (2024) 26807–26827. doi: 10.1021/acsnano.4c07658
P. Shan, J. Liao, J. Li, et al., Chin. Chem. Lett. 35 (2024) 108545. doi: 10.1016/j.cclet.2023.108545
Z. Wen, L. Kang, H. Fu, et al., Carbohydr. Polym. 314 (2023) 120887. doi: 10.1016/j.carbpol.2023.120887
J. Liu, H. Ren, C. Zhang, et al., Small 19 (2023) e2304023. doi: 10.1002/smll.202304023
X. Liu, L. Liu, F. Huang, et al., Food Chem. 470 (2025) 142618. doi: 10.1016/j.foodchem.2024.142618
C.Y. Wang, M. Sun, Z. Fan, J.Z. Du, Chin. J. Polymer Sci. 40 (2022) 1154–1164. doi: 10.1007/s10118-022-2726-0
J. Yang, M. Peng, S. Tan, et al., ACS Cent. Sci. 9 (2023) 1327–1341. doi: 10.1021/acscentsci.3c00227
N.T. Nguyen, B.T. Nguyen, T.N. Ho, et al., Int. J. Biol. Macromol. 269 (2024) 132122. doi: 10.1016/j.ijbiomac.2024.132122
K. Zhang, Y. Liang, Q. Chen, et al., ACS Nano 19 (2025) 27825–27844. doi: 10.1021/acsnano.5c08982
X. Liu, C. Steiger, S. Lin, et al., Nat. Commun. 10 (2019) 493. doi: 10.1038/s41467-019-08355-2
L. Polakova, V. Raus, L. Cuchalova, et al., Int. J. Pharm. 613 (2022) 121392. doi: 10.1016/j.ijpharm.2021.121392
M.K. Coolich, O.L. Lanier, E. Cisneros, N.A. Peppas, J. Control. Release 364 (2023) 216–226. doi: 10.1016/j.jconrel.2023.10.020
J. Qi, Y. Wang, H. Chen, et al., Adv. Sci. 12 (2025) e2407802. doi: 10.1002/advs.202407802
Z. Zhang, Y. Pan, Z. Guo, et al., Bioact. Mater. 33 (2024) 71–84.
X. Xu, H. Liu, J. Guo, et al., Int. J. Pharm. 590 (2020) 119880. doi: 10.1016/j.ijpharm.2020.119880
F. Li, Z. Zhang, X. Wang, et al., Int. J. Biol. Macromol. 289 (2024) 138875.
K.S. Postolovic, M.D. Antonijevic, B. Ljujic, et al., Molecules 27 (2022) 4045. doi: 10.3390/molecules27134045
H. Poursadegh, M.S. Amini-Fazl, S. Javanbakht, F. Kazeminava, Int. J. Biol. Macromol. 254 (2024) 127702. doi: 10.1016/j.ijbiomac.2023.127702
J. Wang, D. Hu, Q. Chen, et al., Mater. Today Bio 20 (2023) 100679. doi: 10.1016/j.mtbio.2023.100679
S. Noureen, S. Noreen, S.A. Ghumman, et al., Eur. J. Pharm. Sci. 189 (2023) 106555. doi: 10.1016/j.ejps.2023.106555
S. Naeem, K. Barkat, M. Shabbir, et al., Drug Dev. Ind. Pharm. 48 (2022) 611–622. doi: 10.1080/03639045.2022.2150773
N. Shahid, A. Erum, M. Zaman, et al., Int. J. Nanomedicine 16 (2021) 6345–6366. doi: 10.2147/ijn.s330186
Y. Yang, Y. Liu, S. Chen, et al., Carbohydr. Polym. 246 (2020) 116617. doi: 10.1016/j.carbpol.2020.116617
X. Wang, Z. Zhang, H. Lei, et al., Int. J. Biol. Macromol. 285 (2024) 138223.
B. Hu, S. Yu, C. Shi, et al., ACS Nano 14 (2020) 2760–2776. doi: 10.1021/acsnano.9b09125
D. Zhong, K. Jin, R. Wang, et al., Adv. Mater. 36 (2024) e2312275. doi: 10.1002/adma.202312275
C. Lu, C. Chang, Y. Zheng, et al., ACS Appl. Mater. Interfaces 16 (2024) 60027–60044. doi: 10.1021/acsami.4c15042
K.Y. Wong, Z. Nie, M.S. Wong, et al., Adv. Mater. 36 (2024) e2404053. doi: 10.1002/adma.202404053
Y. Jing, Y. Zhang, W. Cheng, et al., Int. J. Biol. Macromol. 263 (2024) 130376. doi: 10.1016/j.ijbiomac.2024.130376
H. Zhang, J. Zhang, B. Liu, et al., Adv. Funct. Mater. 34 (2024) 2401064. doi: 10.1002/adfm.202401064
S. Mao, Y. Ren, S. Chen, et al., Carbohyd. Polymers 320 (2023) 121234. doi: 10.1016/j.carbpol.2023.121234
L. Xu, X. Du, Y. Zhou, et al., Mol. Pharm. 20 (2023) 2105–2118. doi: 10.1021/acs.molpharmaceut.2c01062
Z. Li, G. Li, J. Xu, et al., Adv. Mater. 34 (2022) e2109178. doi: 10.1002/adma.202109178
A. Mir, A. Kumar, J. Alam, U. Riaz, Int. J. Biol. Macromol. 252 (2023) 126015. doi: 10.1016/j.ijbiomac.2023.126015
Y. Hu, S. Gao, H. Lu, J.Y. Ying, J. Am. Chem. Soc. 144 (2022) 5461–5470. doi: 10.1021/jacs.1c13426
Y. Hu, J. Liu, Y. Ke, et al., ACS Appl. Mater. Interfaces 16 (2024) 29235–29247. doi: 10.1021/acsami.4c03834
S.H. Weon, Y. Na, J. Han, et al., Gels 10 (2024) 200. doi: 10.3390/gels10030200
R. Feng, M. Wang, Z. Song, et al., Food Hydrocolloids 158 (2025) 110488. doi: 10.1016/j.foodhyd.2024.110488
H. Kumar Chaudhary, P. Singh, K. Niveria, et al., Int. J. Pharm. 662 (2024) 124452. doi: 10.1016/j.ijpharm.2024.124452
F. Lei, F. Zeng, X. Yu, et al., J. Nanobiotechnology 21 (2023) 275. doi: 10.1186/s12951-023-02045-4
G. Zhang, D. Song, R. Ma, et al., Sci. Adv. 10 (2024) eado8222. doi: 10.1126/sciadv.ado8222
L. Huang, J. Wang, L. Kong, et al., Int. J. Biol. Macromol. 222 (2022) 1476–1486. doi: 10.1016/j.ijbiomac.2022.09.247
Y. Peng, X. Luo, X. Wang, et al., Bioact. Mater. 41 (2024) 627–639.
M. Pandey, H. Choudhury, S.K. D/O Segar Singh, et al., Molecules 26 (2021) 2704. doi: 10.3390/molecules26092704
X. Xu, X. Xia, K. Zhang, et al., Sci. Transl. Med. 12 (2020) eaba8014. doi: 10.1126/scitranslmed.aba8014
R. Xie, X. Yan, J. Yu, et al., Biomaterials 309 (2024) 122599. doi: 10.1016/j.biomaterials.2024.122599
H.B. Huang, W. Gong, Y.Y. Hou, et al., J. Agric. Food Chem. 71 (2023) 4016–4028. doi: 10.1021/acs.jafc.2c07777
X. Yang, W. Nie, C. Wang, et al., Biomaterials 308 (2024) 122564. doi: 10.1016/j.biomaterials.2024.122564
J. Qiu, S. Xiang, M. Sun, M. Tan, J. Agr, Food Chem. 71 (2023) 18842–18856. doi: 10.1021/acs.jafc.3c05898
F. Song, J. Gong, Y. Tao, et al., Int. J. Biol. Macromol. 176 (2021) 448–458. doi: 10.1016/j.ijbiomac.2021.02.104
H.T. Hoang, S.H. Jo, Q.T. Phan, et al., Carbohyd. Polymers 260 (2021) 117812. doi: 10.1016/j.carbpol.2021.117812
M. Mamdouh, A. Donia, E. Essa, G.E. Maghraby, Curr. Drug Deliv. 16 (2019) 862–871. doi: 10.2174/1567201816666191014102531
L. Cao, J. Li, B. Parakhonskiy, A.G. Skirtach, Food Chem. 451 (2024) 139205. doi: 10.1016/j.foodchem.2024.139205
W.C. Huang, W. Wang, W. Wang, et al., Engineering 34 (2024) 187–194. doi: 10.1016/j.eng.2023.05.024
X. Ye, T. Chen, Y. Du, et al., Colloids Surf. B: Biointerfaces 246 (2025) 114367. doi: 10.1016/j.colsurfb.2024.114367
J. Xie, P. Yu, Z. Wang, J. Li, Biomacromolecules 23 (2022) 641–660. doi: 10.1021/acs.biomac.1c01647
Y. Sheng, J. Gao, Z.Z. Yin, et al., Carbohydr. Polym. 269 (2021) 118325. doi: 10.1016/j.carbpol.2021.118325
J. Ouyang, B. Deng, B. Zou, et al., J. Am. Chem. Soc. 145 (2023) 12193–12205. doi: 10.1021/jacs.3c02179
I. Fraile-Gutiérrez, S. Iglesias, N. Acosta, J. Revuelta, Int. J. Biol. Macromol. 255 (2024) 127755. doi: 10.1016/j.ijbiomac.2023.127755
X. Wang, H. Gu, H. Zhang, et al., ACS Appl. Mater. Interfaces 13 (2021) 33948–33961. doi: 10.1021/acsami.1c09804
K. Rajpoot, S.K. Jain, Int. J. Biol. Macromol. 151 (2020) 830–844. doi: 10.1016/j.ijbiomac.2020.02.132
R. Grosso, E. Benito, A.I. Carbajo-Gordillo, et al., Int. J. Mol. Sci. 24 (2023) 2281. doi: 10.3390/ijms24032281
K. Silva, D.E.L. de Carvalho, V.M.M. Valente, et al., Int. J. Biol. Macromol. 126 (2019) 359–366. doi: 10.1016/j.ijbiomac.2018.12.136
H. Gong, X. Wang, X. Hu, et al., Biomacromolecules 25 (2024) 1602–1611. doi: 10.1021/acs.biomac.3c01141
W. Zhang, Y. Zhou, Y. Fan, et al., Adv. Mater. 34 (2022) e2105738. doi: 10.1002/adma.202105738
N.A. Mohamed, N.A. Abd El-Ghany, M.M. Abdel-Aziz, Int. J. Biol. Macromol. 181 (2021) 956–965. doi: 10.1016/j.ijbiomac.2021.04.095
Y. Lai, T. Zhang, X. Yin, et al., Acta Pharm. Sin. B 14 (2024) 3184–3204. doi: 10.1016/j.apsb.2024.03.014
Z. Cheng, R. Qing, S. Hao, et al., Regen. Biomater. 8 (2021) rbab008. doi: 10.1093/rb/rbab008
E.J. Heikal, R.M. Kaoud, S. Gad, et al., Pharmaceuticals 16 (2023) 795. doi: 10.3390/ph16060795
L. Xu, E. Bai, Y. Zhu, et al., Pharmaceutics 15 (2023) 257. doi: 10.3390/pharmaceutics15010257
M. Gao, C. Yang, C. Wu, et al., J. Nanobiotechnology 20 (2022) 404. doi: 10.1186/s12951-022-01603-6
Y. Zhu, Y. Wang, G. Xia, et al., Adv. Sci. 10 (2023) e2207418. doi: 10.1002/advs.202207418
R. Luo, J. Liu, Q. Cheng, et al., Sci. Adv. 10 (2024) eado6798. doi: 10.1126/sciadv.ado6798
L. Qiu, R. Shen, L. Wei, et al., J. Nanobiotechnology 21 (2023) 344. doi: 10.1186/s12951-023-02097-6
Y. Ma, S. Gou, Z. Zhu, et al., Adv. Mater. 36 (2024) e2309516. doi: 10.1002/adma.202309516
S. Liu, Y. Cao, L. Ma, et al., J. Control. Release 347 (2022) 544–560. doi: 10.1016/j.jconrel.2022.05.025
G. Zhang, D. Song, R. Ma, et al., Int. J. Biol. Macromol. 273 (2024) 132909. doi: 10.1016/j.ijbiomac.2024.132909
K. Han, J. Nam, J. Xu, et al., Nat. Biomed. Eng. 5 (2021) 1377–1388. doi: 10.1038/s41551-021-00749-2
X. Cao, S. Tao, W. Wang, et al., Nat. Commun. 15 (2024) 8428. doi: 10.1038/s41467-024-52722-7
D. Faizullin, Y. Valiullina, V. Salnikov, et al., Int. J. Mol. Sci. 24 (2023) 926. doi: 10.3390/ijms24020926
W. Li, X. Zhu, X. Zhou, et al., J. Control. Release 334 (2021) 376–388. doi: 10.1016/j.jconrel.2021.04.036
N.M. El-Deeb, O.M. Ibrahim, M.A. Mohamed, et al., Int. J. Biol. Macromol. 205 (2022) 385–395. doi: 10.1016/j.ijbiomac.2022.02.058
M.M. Ghobashy, A.M. Elbarbary, D.E. Hegazy, Carbohydr. Polym. 263 (2021) 117975. doi: 10.1016/j.carbpol.2021.117975
M. Abbasi, M. Sohail, M.U. Minhas, et al., Int. J. Biol. Macromol. 233 (2023) 123585. doi: 10.1016/j.ijbiomac.2023.123585
L. Li, S. He, B. Liao, et al., Research 7 (2024) 0364. doi: 10.34133/research.0364
Y. Cao, S. Liu, Y. Ma, et al., Small 18 (2022) e2203466. doi: 10.1002/smll.202203466
N. Batool, R.M. Sarfraz, A. Mahmood, et al., Gels 8 (2022) 190. doi: 10.3390/gels8030190
S. Md, S. Abdullah, Z.A. Awan, N.A. Alhakamy, J. Pharm. Sci. 111 (2022) 3155–3164. doi: 10.1016/j.xphs.2022.08.019
W. Li, J.X. Fan, J.Y. Qiao, et al., J. Control. Release 356 (2023) 59–71. doi: 10.1016/j.jconrel.2023.02.028
P. Zhu, L. Meng, Y. Shu, et al., Carbohydr. Polym. 329 (2024) 121797. doi: 10.1016/j.carbpol.2024.121797
M. Madaghiele, C. Demitri, I. Surano, et al., Sci. Rep. 11 (2021) 21394. doi: 10.1038/s41598-021-00884-5
A. Silvestri, A. Gil-Gomez, M. Vitale, et al., Cell Rep. Med. 4 (2023) 101235. doi: 10.1016/j.xcrm.2023.101235
Y. Le, H. Li, X. Liao, et al., Food Res. Int. 190 (2024) 114560. doi: 10.1016/j.foodres.2024.114560
S. Chen, Q. Miao, Y. Liu, et al., Int. J. Biol. Macromol. 253 (2023) 126915. doi: 10.1016/j.ijbiomac.2023.126915
H. Wu, J. Nan, L. Yang, et al., J. Control. Release 353 (2023) 51–62. doi: 10.1016/j.jconrel.2022.11.032
Y. Yang, S. Chen, Y. Liu, et al., Biomed. Pharmacother. 133 (2021) 110941. doi: 10.1016/j.biopha.2020.110941
C. Ren, D. Zhong, Y. Qi, et al., ACS Nano 17 (2023) 14161–14175. doi: 10.1021/acsnano.3c04897
R. Ying, W. Wang, R. Chen, et al., Biomacromolecules 25 (2024) 7446–7458. doi: 10.1021/acs.biomac.4c01093
Y. Zhou, Z. Chen, D. Zhao, et al., Adv. Mater. 33 (2021) e2102044. doi: 10.1002/adma.202102044
X. Qu, Z. Xie, J. Zhang, et al., Small (2024) e2409936.
R. Peng, C. Song, S. Gou, et al., Pharmacol. Res. 202 (2024) 107121. doi: 10.1016/j.phrs.2024.107121
J. Li, G. Wei, G. Liu, et al., Adv. Sci. 10 (2023) e2207381. doi: 10.1002/advs.202207381
J. Su, P. Wang, W. Zhou, et al., Nat. Nanotechnol. 19 (2024) 1168–1177. doi: 10.1038/s41565-024-01657-7
C. Liu, Q. Ye, S. Hua, et al., Nano Today 53 (2023) 102034. doi: 10.1016/j.nantod.2023.102034
N.A.N. Hanafy, Int. J. Biol. Macromol. 183 (2021) 171–181. doi: 10.1016/j.ijbiomac.2021.04.131
P. Sagar, V. Singh, R. Gupta, et al., ACS Appl. Bio. Mater. 4 (2021) 7467–7484. doi: 10.1021/acsabm.1c00720
A. Liu, M. He, C. Liu, et al., J. Agric. Food Chem. 72 (2024) 6118–6132. doi: 10.1021/acs.jafc.3c08697
D.W. Zheng, K.W. Chen, J.H. Yan, et al., Mater. Today 58 (2022) 30–40. doi: 10.1016/j.mattod.2022.07.014
Y. Wu, Z. Tang, S. Du, et al., Int. J. Pharm. 658 (2024) 124225. doi: 10.1016/j.ijpharm.2024.124225
K. Han, F. Xie, O. Animasahun, et al., Nat. Mater. 23 (2024) 1444–1455. doi: 10.1038/s41563-024-01909-w
X. Lin, L. Miao, X. Wang, H. Tian, Colloids Surf. B: Biointerfaces. 195 (2020) 111200. doi: 10.1016/j.colsurfb.2020.111200
M. Sun, Y. Shi, B. Lei, et al., Vet. Res. 55 (2024) 153. doi: 10.1186/s13567-024-01411-w
Y. Tang, Y. Du, J. Ye, et al., Adv. Mater. 36 (2023) e2310492.
G. Liu, Y. Zhou, Z. Xu, et al., Chin. Chem. Lett. 34 (2023) 107705. doi: 10.1016/j.cclet.2022.07.048
I. Dmour, Carbohydr. Polym. 343 (2024) 122486. doi: 10.1016/j.carbpol.2024.122486
H. Tolabi, N. Davari, M. Khajehmohammadi, et al., Adv. Mater. 35 (2023) e2208852. doi: 10.1002/adma.202208852
J. Zheng, R. Fan, H. Wu, et al., Nat. Commun. 10 (2019) 1604. doi: 10.1038/s41467-019-09601-3
W. Luo, Z. Yang, J. Zheng, et al., ACS Nano 18 (2024) 28894–28909. doi: 10.1021/acsnano.4c09097

Figure 2 Schematic diagram of synthesis principle of oral hydrogels. (A) Schematic diagram of hemicellulose/graphene oxide composite hydrogel through physical crosslinking. Copied with permission [32]. Copyright 2025, Elsevier. (B) Chemical crosslinking is achieved through (a) photoinitiation. Copied with permission [35]. Copyright 2023, Elsevier. (b) Ether bond formation reaction. Copied with permission [40]. Copyright 2025, Elsevier. (C) Self-assembled microalgae/rhein hydrogels. Copied with permission [42]. Copyright 2024, John Wiley and Sons. (D) Sodium alginate and protocatechuic acid form metal phenol network hydrogels through rapid self-assembly of Ca2+, Fe3+. Copied with permission [47]. Copyright 2023, Elsevier.

Figure 3 Schematic diagram of pH response, ROS response, enzyme response, and high adhesion of oral intelligent hydrogels.

Figure 4 (A) Schematic diagram of the preparation of Dex-sBSA self-healing hydrogels and photos of its self-healing characteristics. Copied with permission [65]. Copyright 2023, American Chemical Society. (B) Scheme for forming polyelectrolyte hydrogels between PAA, norbornene functionalized chitosan (CsNb), and temperature-sensitive monomer bisTz-PNIPAM. Copied with permission [67]. Copyright 2021, Elsevier.

Figure 5 (A) With the stimulus of simulated gastric fluid (SGF, pH 1.2), iAPA was deionized, and a stable hydrogel could be formed owing to the restoration of hydrophobicity-assisted multiple hydrogen bonds as non-covalent crosslinking points in the network. Copied with permission [62]. Copyright 2024, Elsevier. (B) SA/PASP@CaCO3 hydrogels loaded with baicalin inhibits oxidative stress through NRF2/HO-1 signaling pathway and is used to treat three gastric ulcer models. Copied with permission [86]. Copyright 2023, the Author(s). (C) Application of oral hydrogels in gastric diseases. Oral hydrogels can form an adhesive barrier on the gastric wall and play a role in delivering therapeutic drugs. At the same time, the hydrogels can also be designed as a multi-functional platform, and the decomposed components (such as metal ions) can be used to treat stomach diseases.

Figure 6 Schematic diagram of oral hydrogels for treatment of inflammatory bowel disease. Natural polymers, as drug carriers, can provide sustained anti-inflammatory support and intestinal repair due to their inherent properties.

 扫一扫看文章
扫一扫看文章

扫一扫关注我们
 DownLoad:
DownLoad:

 下载:
下载:

 下载:
下载: