Citation:
Longhui Hao, Yi Zhang, Ying Sun, Yanqi Han, Jun Ye, Hongliang Wang, Lili Gao, Dong Wang, Yue Gao, Yanfang Yang, Yuling Liu. Advances in nano-delivery systems for targeted natural product delivery to specific skin layers in disease therapy and skin care[J]. Chinese Chemical Letters,
2026, 37(7): 111597.
doi:
10.1016/j.cclet.2025.111597
Advances in nano-delivery systems for targeted natural product delivery to specific skin layers in disease therapy and skin care
English
Advances in nano-delivery systems for targeted natural product delivery to specific skin layers in disease therapy and skin care
Shenyang Pharmaceutical University, Shenyang 110016, China
b.
Beijing Key Laboratory of Drug Delivery Technology and Novel Formulation, Institute of Materia Medica, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing 100050, China
Received Date:
26 March 2025 Accepted Date:
16 July 2025 Revised Date:
15 July 2025 Available Online:
15 July 2026
Abstract:
Compared to synthetic chemical compounds, plant extracts derived from natural sources have emerged as the "new favorites" in the treatment and care of skin diseases due to their distinct advantages, including being environmentally friendly, sustainable, and safe. However, challenges such as poor solubility, limited permeability, and the barrier function of the stratum corneum significantly restrict the application of natural products in dermal drug delivery. Fortunately, advancements in nanotechnology offer promising solutions to overcome these challenges. Different skin diseases and treatments require the precise delivery of natural active ingredients to specific skin layers, and the unique structure of nanocarriers enables targeted delivery to achieve desired therapeutic outcomes. This paper begins by exploring the pathogenesis and therapeutic targets of common skin conditions, including atopic dermatitis (AD), psoriasis, decubitus ulcers, diabetic foot ulcers (DFUs), as well as applications in antioxidant therapies and anti-aging strategies. Furthermore, it provides a detailed overview of the depths and locations within the skin where active compounds must be delivered to exert their effects effectively. Subsequently, this review categorizes and examines natural products based on their therapeutic effects on various skin diseases. It then highlights the skin depths and specific sites that can be targeted by different delivery systems designed to enhance skin permeability, tailored to meet the needs of skin disease treatment or care. By addressing these aspects, this review aims to provide a valuable reference for advancing research on nano-delivery systems in the field of topical skin drug delivery for the treatment and management of skin diseases.
In recent years, the rapid growth of the pharmaceutical industry has led to greater focus on functional topical skin products. With rising needs for treating skin diseases and improving appearance, skincare has become a multidisciplinary field involving dermatology, biology, and pharmaceutical science. Modern skincare products are no longer just for beauty, they now also offer therapeutic benefits, helping treat specific skin problems and bridging the gap between cosmetics and medicine [1].
Although many synthetic drugs are used to treat skin diseases, they often cause side effects. In contrast, natural bioactive compounds from plants are safer and work on multiple targets. They have anti-cancer, anti-inflammatory, antibacterial, and anti-aging effects. Common types include polyphenols, flavonoids, terpenes, glycosides, and alkaloids, often found in traditional Chinese medicine. For example, tea polyphenols and curcumin help reduce inflammation, chlorogenic acid and arbutin help whiten skin, and asiaticoside and β-glucan help heal wounds and eczema. These natural compounds are safer and better for long-term use than synthetic drugs. However, poor solubility, low permeability, and the skin barrier still limit their effectiveness [2]. Drug delivery systems (DDS) like nanoparticles, nanoemulsions (NEs), liposomes, nanocrystals, and liquid crystal (LC) emulsions (LCEs) help overcome these challenges.
As shown in Fig. 1A, the skin consists of two primary layers: the epidermis and the dermis. The epidermis is subdivided into four layers: stratum corneum, stratum granulosum, stratum spinosum, and stratum basale [3]. These tightly connected layers form an effective barrier against external stimuli [4]. The dermis, beneath the epidermis, contains fibroblasts, immune cells, and an extracellular matrix (ECM) rich in collagen and elastin fibers, providing structural support and regulating immune cell migration. Maintaining the integrity and function of the skin, including the sebaceous membrane, stratum corneum, and each epidermal layer, is key to improving skin conditions. However, due to the skin's barrier function, most topical preparations act mainly on the epidermis, particularly the basal layer, limiting their effects on deeper skin layers [5]. Only certain ultrafine molecules, like some essential oils, can penetrate into the dermis, but their effects are minimal due to low permeability (Fig. 1B) [6]. Therefore, precise delivery of natural active ingredients to target skin layers is critical to maximize therapeutic benefits.
Figure 1
Figure 1.
(A) Structure of the skin, including the epidermis, dermis (papillary and reticular layers), and hypodermis, with key adnexal structures indicated. Copied with permission [3]. Copyright 2015, American Society for Clinical Investigation. (B) Schematic diagram of the pathway of drug penetration through the skin. Reproduced with permission [6]. Copyright 2011, Elsevier.
This thesis reviews recent advances in delivery systems for natural active ingredients in the treatment and care of skin diseases. These systems play a critical role in overcoming the skin's barrier, enabling active compounds to effectively reach their target layers and exert therapeutic effects. To provide a comprehensive understanding, the review first explores the pathogenesis of common skin conditions, such as inflammation, wounds, and aging, to identify the specific skin layers that require intervention. It then classifies natural active ingredients based on their mechanisms of action in skin treatment and care. Finally, it summarizes the progress in novel delivery systems, focusing on their delivery depth, action mechanisms, and applications for different skin disorders. This review aims to offer valuable references for guiding the clinical and cosmetic application of natural actives and for selecting delivery strategies tailored to targeted skin structures.
2.
Pathogenesis of skin-related diseases
Current research shows that managing skin diseases requires targeting multiple factors, such as repairing the skin barrier, reducing inflammation, controlling sebum, promoting tissue repair, fighting oxidation, and preventing infection. For example, immune-related conditions like atopic dermatitis (AD) and psoriasis involve chronic inflammation and a damaged skin barrier, so treatments focus on reducing inflammation, restoring the barrier, and supporting healing. In contrast, acne is linked to too much sebum, clogged pores, bacteria, and local inflammation, so therapies aim to control oil, fight microbes, reduce inflammation, and boost collagen to avoid scars. Chronic wounds like pressure sores, diabetic foot ulcers, and surgical wounds need treatments that prevent infection, rebuild tissue, promote blood vessel growth, and speed up healing. In addition, skincare products now often include antioxidants, anti-inflammatory agents, whitening ingredients, moisturizers, and anti-aging compounds to fight oxidative stress, dark spots, water loss, and skin aging—helping to keep the skin healthy and improve appearance.
Therefore, a comprehensive understanding of disease mechanisms and therapeutic targets is essential for the effective use of natural compounds and the development of appropriate delivery systems. This paper outlines key mechanisms, including barrier repair, inflammation modulation, tissue regeneration, and antioxidant and antimicrobial effects, to inform mechanism-based skincare strategies and enhance clinical outcomes. Table 1 summarizes the discussed skin disorders, their underlying mechanisms, and corresponding therapeutic approaches.
Table 1
Table 1.
Mechanisms and care strategies for different types of skin diseases.
2.1
Immune-mediated skin diseases and care strategies
2.1.1
AD
AD is a common inflammatory skin disorder, often accompanied by subtypes such as contact dermatitis and seborrheic dermatitis. It is characterized by erythema, pruritus, dryness, scaling, and, in severe cases, oozing. AD primarily affects the epidermis, especially the stratum corneum, impairing the skin barrier function and increasing susceptibility to dryness, infection, and irritation [7,8]. The pathogenesis of AD involves skin barrier dysfunction, immune dysregulation, microbial imbalance, and hypersensitivity reactions. As shown in Fig. 2, Th2-mediated immune responses play a central role, with overexpression of interleukin-4 (IL-4), IL-5, and IL-13 promoting inflammation and pruritus. Barrier protein deficiency (e.g., filaggrin) and lipid abnormalities further weaken skin defense. Microbiome disturbances, particularly Staphylococcus aureus overgrowth, release toxins that aggravate inflammation. Additionally, allergens activate IgE and mast cells, triggering histamine release and amplifying symptoms [9-12].
Figure 2
Figure 2.
Pathogenesis, key mechanisms, and pathophysiology of AD. Copied with permission [12]. Copyright 2020, BMJ Publishing Group.
For patients with mild to moderate symptoms, topical medications are the first-line choice. These include topical corticosteroids (such as hydrocortisone butyrate cream and fluocinolone cream) to alleviate erythema and pruritus, and calcineurin inhibitors (such as tacrolimus ointment and pimecrolimus cream) which are suitable for sensitive areas like the face [13,14]. In addition, barrier-repair moisturizers containing ceramides are essential to maintain skin hydration and integrity. For patients with moderate to severe or recurrent symptoms, systemic therapies are employed. Oral antihistamines (such as loratadine and cetirizine) help control pruritus, especially nocturnal itching [15]. Systemic corticosteroids (such as prednisone) may be used during acute flares, although long-term use is not recommended due to potential side effects [16]. Immunosuppressive agents like cyclosporine A and methotrexate are considered for refractory cases. In recent years, biologics such as dupilumab have been widely applied in moderate-to-severe cases. Furthermore, small molecule drugs including Janus kinase (JAK) inhibitors like baricitinib, upadacitinib, and abrocitinib have been approved for adult and adolescent patients [17].
In addition to conventional therapies, natural agents such as chlorogenic acid and glycyrrhizic acid have shown promising anti-inflammatory and barrier-repairing properties, and are increasingly being explored as adjunct treatments in advanced topical delivery systems to enhance efficacy and skin penetration. Moreover, some traditional Chinese medicine formulations containing ingredients like Sophora flavescens or Rehmannia are also applied topically, though their clinical effectiveness and safety still require further validation [18].
2.1.2
Psoriasis
Psoriasis is a common chronic inflammatory skin disease characterized by well-demarcated erythematous plaques with silvery-white scales, often accompanied by pruritus and discomfort. These lesions primarily result from excessive proliferation and abnormal differentiation of keratinocytes, leading to epidermal thickening and plaque formation, while dermal inflammation contributes to erythema and irritation [19]. The pathogenesis involves immune dysregulation, with overactivation of T lymphocytes, particularly Th1 and Th17 subsets, driving elevated secretion of interferon-γ (IFN-γ), IL-17, and IL-22, which promote inflammation and keratinocyte hyperproliferation. Additionally, neutrophil infiltration, accelerated epidermal turnover, and genetic susceptibility (e.g., HLA-C06*) further contribute to disease progression [20-22], as illustrated in Fig. S1A (Supporting information).
Clinically, psoriasis treatment is stratified by disease severity and encompasses topical agents, systemic medications, biologics, and phototherapy. For mild cases, topical corticosteroids (e.g., hydrocortisone butyrate, halometasone) are widely used to relieve inflammation and itching, while tazarotene, a topical retinoid, is prescribed to regulate keratinocyte differentiation [23]. Calcineurin inhibitors such as tacrolimus are particularly suited for sensitive areas like the face. Moderate-to-severe cases often require systemic treatments, including methotrexate, cyclosporine A, and acitretin, which have demonstrated clinical efficacy [24]. In recent years, biologic therapies have become central to management, targeting key immune pathways with agents such as IL-17 inhibitors, IL-23 inhibitors, and tumor necrosis factor-α (TNF-α) blockers. JAK inhibitors like tofacitinib are also employed in patients intolerant to conventional options. Phototherapy, including narrow-band ultraviolet B (NB-UVB) and 308 nm excimer laser, is frequently utilized for widespread lesions [25].
Traditional Chinese medicine therapies, including indigo naturalis ointment and Sophora flavescens (Kushen) decoction, have also gained attention as adjunctive treatments due to their anti-inflammatory and lesion-relieving properties. Similarly, natural bioactive compounds such as azurin, baicalin, chlorogenic acid, and glycyrrhizic acid have shown potential in regulating inflammation and oxidative stress, contributing to a more comprehensive therapeutic strategy. As demonstrated in Fig. S1B (Supporting information), Jeon et al. demonstrated that rhododendrin significantly attenuates Toll-like receptor 7 (TLR7)-mediated psoriasis-like skin inflammation in mice by inhibiting nuclear factor-kappa B (NF-κB) and interferon regulatory factor 7 (IRF7) signaling pathways, underscoring its promise as a natural anti-inflammatory agent [26].
2.2
Sebaceous gland disorders: Mechanisms and therapeutic approaches
Sebaceous gland dysfunction underlies the pathogenesis of various skin diseases, with acne being the most common (Fig. S2A in Supporting information). Acne is a chronic inflammatory skin disorder that primarily affects the sebaceous glands and hair follicles, presenting as papules, pustules, nodules, and cysts [27], primarily on the face, back, and chest. Its development involves excessive sebum secretion, abnormal follicular keratinization, microbial colonization, and inflammation. Androgens bind to their receptors and activate 5α-reductase, converting testosterone into dihydrotestosterone (DHT), which stimulates sebaceous glands to produce more sebum [28,29]. Concurrently, aberrant keratinocyte proliferation leads to follicular plugging and comedone formation. The anaerobic, lipid-rich environment promotes the growth of Cutibacterium acnes (C. acnes), which triggers inflammatory cascades by releasing pro-inflammatory mediators such as IL-1, IL-8, and TNF-α via activation of the NF-κB pathway [30]. TLR-2 activation and histamine signaling further contribute to inflammation, redness, and pruritus [31,32]. The key role of bacterial infection is also supported by mouse models, where injection of Acinetobacter induces acne-like lesions, while controls show only mild swelling (Fig. S2B in Supporting information).
Currently, the clinical treatment of acne focuses on four key aspects: excessive sebum production, abnormal follicular keratinization, bacterial infection, and inflammation. To control hyperactive sebaceous gland activity, retinoids and anti-androgenic agents are commonly employed to suppress sebum production [33]. Abnormal follicular keratinization is managed using retinoids and azelaic acid, which regulate keratinocyte differentiation and prevent follicular obstruction [34]. In terms of bacterial infection, antibiotics such as clindamycin and erythromycin, along with benzoyl peroxide, are widely used to reduce C. acnes populations [35]. Meanwhile, inflammation plays a pivotal role in acne pathogenesis. Park et al. demonstrated that the TLR4/myeloid differentiation factor 2 (MD-2) complex is critically involved in lipopolysaccharide (LPS)-induced immune exacerbation, and specific peptides targeting this complex can effectively attenuate inflammatory responses in vivo [36]. Based on these findings, acne-associated inflammation can be alleviated by nonsteroidal anti-inflammatory drugs (NSAIDs), NF-κB pathway inhibitors, TLR2 antagonists, and antihistamines, which collectively help to relieve erythema, pruritus, and local inflammatory symptoms.
2.3
Skin injury and chronic wound healing
The wound healing process is generally divided into four sequential phases: hemostasis, inflammation, proliferation, and remodeling [37]. In the hemostasis phase, vasoconstriction and platelet aggregation initiate clot formation through the release of platelet-derived growth factor (PDGF) and transforming growth factor-β (TGF-β), which activate coagulation cascades and form a fibrin scaffold for subsequent cell migration [38,39]. During inflammation, neutrophils and macrophages sequentially infiltrate the wound site, clearing debris and secreting pro-inflammatory and pro-healing cytokines such as TNF-α, IL-6, vascular endothelial growth factor (VEGF), and fibroblast growth factor (FGF). These cytokines, via activation of pathways like NF-κB, promote immune cell recruitment and infection control [40]. The proliferative phase features endothelial and fibroblast activation, with VEGF and FGF driving angiogenesis, and PDGF and TGF-β promoting fibroblast-mediated ECM and collagen deposition. Concurrently, keratinocytes and epithelial cells migrate inward to re-establish the skin barrier [41]. In the remodeling phase, type Ⅲ collagen is gradually replaced by type Ⅰ collagen to enhance tensile strength, while matrix metalloproteinases (MMPs) degrade excess ECM to regulate matrix turnover. Simultaneously, redundant vasculature regresses and the wound contracts, restoring skin integrity and barrier function [42].
2.3.1
Decubitus ulcers
Decubitus ulcers or pressure sores are chronic wounds caused by prolonged pressure, leading to ischemic necrosis of the skin and deeper tissues, frequently seen in bedridden or immobile patients [43]. Their pathogenesis involves a cascade of pathological events: sustained pressure induces local ischemia and hypoxia, triggering chronic inflammation (mainly mediated by TNF-α, IL-6, and IL-1β), persistent NF-κB pathway activation, and excessive reactive oxygen species (ROS) production [44]. These processes lead to continuous tissue damage, ECM degradation, and impaired healing. Clinically, treatment focuses on tissue regeneration, anti-inflammation, antioxidation, and infection control. Mesenchymal stem cells (MSCs) facilitate angiogenesis and tissue repair via VEGF, HGF, and exosome (EXO) secretion [45], TGF-β promotes collagen synthesis, while MMP activity must be controlled to prevent excessive ECM breakdown [46]. ECM-supporting agents like hyaluronic acid and collagen aid in structural repair. Anti-inflammatory agents targeting TNF-α, IL-6, IL-1β, and NF-κB signaling help stabilize the wound environment [47]. Antioxidants such as vitamin C (VC), VE, N-acetylcysteine (NAC), and superoxide dismutase (SOD) mitigate ROS-induced damage and accelerate healing [48]. Given the high risk of infection, broad-spectrum antibiotics and antimicrobial dressings are essential for preventing bacterial colonization and promoting recovery [49].
Pressure ulcers are commonly treated with pressure relief, wound cleaning, suitable dressings, infection control, and tissue repair. Hydrocolloids, foams, hydrogels, or silver-based dressings are selected based on wound type, while severe cases may require debridement or surgical interventions [50]. Adjunctive therapies like negative pressure wound therapy (NPWT), platelet-rich plasma (PRP), and topical agents containing hyaluronic acid or growth factors can support healing [51]. Natural compounds such as honey, aloe vera, curcumin, asiaticoside, and green tea extract have shown anti-inflammatory and wound-healing effects [52]. They help reduce inflammation, maintain moisture, and promote tissue regeneration [53]. Clinical and animal studies suggest these agents, especially when combined with advanced delivery systems, may further improve therapeutic outcomes.
2.3.2
DFUs
DFUs are common complications in patients with diabetes mellitus, typically presenting as skin breakdowns or ulcers on the feet. They are mainly caused by high blood sugar, nerve damage, and poor blood flow (Fig. S3A in Supporting information) [54]. DFUs affect the dermis and deeper tissues. Even small injuries can lead to infection, tissue death, or amputation due to poor circulation and loss of sensation [55]. DFUs develop through several related factors. High blood sugar causes oxidative stress and forms harmful compounds (AGEs), which damage blood vessels, slow new blood vessel growth, and trigger long-lasting inflammation through the RAGE pathway [56]. Nerve damage lowers pain sensitivity, making injuries go unnoticed and easier to infect [57]. Poor blood flow due to narrowed arteries leads to low oxygen and nutrients, which slows healing [58]. Weak immune responses raise the risk of infection [59], and reduced function of skin cells like keratinocytes and fibroblasts delays repair [60]. A comparison of normal and diabetic wound healing processes is illustrated in Fig. S3B (Supporting information).
DFUs are caused by long-term high blood sugar, which damages nerves and blood vessels, leading to slow healing and high infection risk. Treatment focuses on controlling blood sugar and improving metabolism, while also restoring blood flow through drugs, surgery, or other vascular treatments [61]. Wound care includes debridement, infection control, and using dressings with antimicrobial or healing properties, like silver-based or bioactive materials, which are better than regular wet dressings [62]. For severe or deep wounds, oxygen therapy and skin grafts may help healing [63,64]. Cell therapies, such as using MSCs, are also being explored to support blood vessel growth and tissue repair in DFUs [65].
2.3.3
Surgical wounds
Wounds are defined as disruptions in the continuity of the skin and underlying tissues, typically caused by mechanical forces. The size and shape of a wound depend on the nature of the force, the site of injury, and the direction in which the force is applied [66]. Surgical wounds refer to incisions made during surgical procedures, typically involving the epidermis and dermis, and in some cases extending to subcutaneous tissue, muscle, or internal organs. As the dermis is rich in blood vessels and nerves, such incisions may compromise local circulation and sensory function, potentially impairing the healing process. Reduced blood flow, infection, and postoperative complications are common factors that can delay wound healing [67].
Current treatments primarily include standardized suturing techniques, sterile dressings to prevent infection, and prophylactic use of antibiotics. For complex or slow-healing surgical wounds, clinical approaches such as NPWT, PRP injections, and the application of bioengineered skin substitutes have shown significant therapeutic benefits. NPWT, in particular, is widely used in managing deep or exudative wounds after orthopedic and abdominal surgeries, helping to reduce edema, promote granulation tissue formation, and improve perfusion [68]. Bioactive hydrogels and tissue-engineered dressings embedded with growth factors or antimicrobial agents are also increasingly utilized in hospitals for postoperative wound care [69]. Additionally, natural plant-based preparations are being applied as adjunctive therapies. For example, ointments containing Calendula officinalis or Centella asiatica extracts are used in post-surgical wound dressings for their anti-inflammatory and collagen-stimulating effects [70]. Gel is frequently applied to surgical incisions to promote hydration and epithelial regeneration. These botanical agents contribute to wound repair by reducing inflammation, enhancing angiogenesis, and supporting cell proliferation, thereby improving clinical outcomes in surgical wound healing [71].
2.4
Functional skincare strategies and mechanistic insights
2.4.1
Anti-inflammatory and antioxidant mechanisms in skincare
Under oxidative stress triggered by UV radiation, pollutants, or microbial invasion, ROS accumulate in the skin and activate key antioxidant and anti-inflammatory pathways [72]. Mechanistically, ROS stimulate the dissociation of nuclear factor (erythroid-derived 2)-like 2 (Nrf2) from Keap1, promoting its nuclear translocation and subsequent upregulation of antioxidant enzymes such as SOD and glutathione peroxidase (GPx) [73], as shown in Fig. S4A (Supporting information). Meanwhile, Nrf2 inhibits NF‑κB signaling, reducing the expression of pro‑inflammatory cytokines like IL‑1β and TNF‑α [74]. The phosphatidylinositol 3-kinase/protein kinase B (PI3K/PKB) pathway further enhances Nrf2 activity and suppresses NF‑κB, while cortisol from the hypothalamic–pituitary–adrenal (HPA) axis also contributes to Nrf2 activation [75,76]. At the tissue level, keratinocytes in the basal layer and stratum corneum provide the first line of defense against exogenous oxidative insults via enzymatic antioxidants and physical barrier functions [77], while the dermis contributes structural support, nutrient delivery, and immunoregulatory capacity through its vasculature and appendage structures [78], as shown in Fig. S4B (Supporting information).
Clinically, treatments for oxidative stress-related skin problems often combine antioxidants and anti-inflammatory agents. Common topical antioxidants include VC, VE, coenzyme Q10, and polyphenols. These are added to creams and serums to fight ROS and improve skin health. Nrf2 activators and PI3K/Akt pathway modulators, though still being studied, may boost the skin's natural antioxidant defenses and reduce inflammation. NF-κB inhibitors, such as caffeic acid derivatives and corticosteroids, help lower inflammatory mediator levels [79,80]. Plant extracts like Centella asiatica (for scars), Calendula officinalis (for wound healing), and Camellia sinensis (for anti-aging) are used widely in skincare due to their antioxidant, antimicrobial, and collagen-boosting effects. Glucocorticoids, used topically or systemically, are common for inflammation control. Also, regulating the HPA axis, through stress-reducing methods or adaptogenic skincare, is being explored as a supportive strategy [75,76].
2.4.2
Whitening and pigmentation modulation pathways
Skin pigmentation is mainly regulated by melanogenesis-related signaling pathways, with key mechanisms including inhibition of tyrosinase activity, antioxidation, modulation of melanin transport and degradation, and melanocyte apoptosis [81]. Upon UV exposure, α-MSH secreted by the anterior pituitary binds to melanocortin 1 receptor (MC1R) on melanocytes, activating the cyclic adenosine monophosphate/protein kinase A/cAMP response element-binding protein (cAMP/PKA/CREB) pathway and upregulating microphthalmia-associated transcription factor (MITF) expression [82]. In parallel, UV-stimulated keratinocytes release endothelin-1 (ET-1), which activates the mitogen-activated protein kinase/extracellular signal-regulated kinase (MAPK/ERK) pathway, while the PI3K/Akt pathway further stabilizes MITF via glycogen synthase kinase-3β (GSK-3β) inhibition [83]. Dysregulation of these pathways contributes to pigmentary disorders such as melasma, which is characterized by the overexpression of MC1R, MITF, and ET-1, and vitiligo, which is associated with melanocyte apoptosis and impaired MITF signaling [84,85].
Melanin is produced by melanocytes in the basal layer of the epidermis and transferred to surrounding keratinocytes through dendritic processes [86]. This layer is essential for melanin synthesis and pigment distribution. Most skin-lightening strategies target the epidermis to inhibit melanin production, accelerate its breakdown, or regulate dispersion for a more even tone. Clinically, hyperpigmentation conditions such as melasma are treated with tyrosinase inhibitors (e.g., hydroquinone, kojic acid, arbutin), exfoliants (e.g., glycolic acid, azelaic acid), and retinoids to enhance pigment turnover [87]. Combination therapies like hydroquinone with tretinoin and corticosteroids (Kligman's formula) are often used to boost efficacy and reduce side effects [88]. For stubborn cases, in-office procedures such as chemical peels, laser treatments, or intense pulsed light (IPL) are common. Vitiligo therapies focus on stimulating repigmentation via melanocyte activation and migration, using topical corticosteroids, calcineurin inhibitors, and narrowband UVB phototherapy [89]. Autologous melanocyte transplantation may be considered for stable localized lesions [90]. Regulation of MITF and its signaling pathways plays a key role in both hyperpigmentation and depigmentation, offering a molecular basis for developing targeted treatments [91].
2.4.3
Skin hydration, sebum balance, and barrier function maintenance
Skin moisturization and water-oil balance depend on a barrier formed by natural moisturizing factors (NMFs) and the sebaceous membrane, which jointly prevent excessive water evaporation. Sebum, composed of lipids secreted by sebaceous glands and sweat, forms a protective film on the skin surface to reduce TEWL [92]. Structurally, the stratum corneum contains abundant NMFs (e.g., amino acids, lactates, urea), while the dermis is rich in water, collagen, and hyaluronic acid, providing elasticity and moisture retention. Sebaceous glands within the dermis regulate lipid secretion to maintain hydration and prevent excessive oiliness. Several signaling pathways coordinate this regulation: the PI3K/Akt pathway facilitates the membrane redistribution of aquaporins (especially AQP3), promoting intracellular water transport and osmotic stability while enhancing lipid synthesis through downstream enzyme activation [93,94]; AMPK modulates lipid production in energy-deficient states by inhibiting fatty acid synthesis and adjusting cholesterol metabolism [95]; the mammalian target of rapamycin (mTOR) stimulates sebocyte growth and lipogenesis [96]; NF-κB indirectly suppresses sebum secretion by mediating inflammatory responses [97]; and Nrf2-Keap1 improves barrier function and corrects sebaceous gland hyperactivity under oxidative stress [98]. These pathways jointly maintain skin hydration, lipid balance, and structural integrity [99].
In clinical practice, skin dryness and oil-water imbalance are usually treated with moisturizers, oil-control products, and functional drugs. Moisturizers often include ingredients like glycerin, hyaluronic acid, ceramides, and natural moisturizing factors (NMFs), which help strengthen the skin barrier, reduce water loss, and increase hydration [100]. They are commonly made into creams, lotions, or gels for dry or sensitive skin. Urea creams (5 %–10 %) are also widely used to soften skin, improve moisture, and relieve dryness and eczema symptoms. Oil-control products often contain salicylic acid, azelaic acid, or niacinamide. These ingredients help reduce sebum, clear pores, and are helpful for oily or acne-prone skin [101]. They come in forms like serums, emulsions, and cleansers. Some products combine multiple ingredients, such as niacinamide with zinc PCA, to better balance skin oil and water. In addition, topical products with active ingredients like metformin, hyaluronic acid complexes, or polyphenols can target signaling pathways like AMPK, PI3K/Akt, or Nrf2. These help repair the skin barrier, improve oil-water balance, and support overall skin health [102,103]. They are used in both cosmetic care and clinical settings, especially for skin damaged by aging, inflammation, or environmental stress.
2.4.4
Anti-aging mechanisms and skincare approaches
Skin anti-aging strategies primarily involve five interrelated mechanisms. First, the regulation of oxidative stress plays a central role, where free radical scavenging, particularly ROS, activates the Nrf2-Keap1 and MAPK pathways. Upon oxidative stimulation, Nrf2 dissociates from Keap1 and enters the nucleus to initiate the transcription of antioxidant genes (e.g., HO-1, NQO1, glutathione S-transferases (GST)), while MAPKs (ERK, c-Jun N-terminal kinase (JNK), p38) regulate stress responses and antioxidant defenses [104,105]. Second, ECM remodeling is mediated by the TGF-β/SMAD pathway, which promotes collagen synthesis and fibroblast activity. Simultaneously, anti-aging compounds can enhance tissue inhibitor of metalloproteinases (TIMP) expression to inhibit MMPs, thereby reducing collagen degradation [106,107]. Third, the clearance of senescent cells is governed by the p53/p21 axis, where p53-induced p21 mediates cell cycle arrest or apoptosis, preserving skin homeostasis [108]. Fourth, the inhibition of pro-inflammatory signaling via NF-κB and JAK/STAT pathways helps suppress cytokines such as IL-1, IL-6, and TNF-α, contributing to anti-inflammatory and anti-aging effects [109]. Lastly, targeting glycation processes, particularly the accumulation of AGEs and their interaction with RAGE, can reduce collagen cross-linking and downstream NF-κB-mediated oxidative stress and inflammation, offering another crucial approach for mitigating skin aging [110].
Clinically, skin anti-aging treatments primarily encompass pharmacological, injectable, and device-based approaches. Pharmacological treatments commonly employ topical retinoids, VC, and polyphenolic antioxidants, which modulate oxidative stress, promote collagen production, and exert anti-inflammatory effects [111]. Injectable therapies, including botulinum toxin, hyaluronic acid, peptides, and autologous PRP, effectively reduce wrinkles and enhance skin hydration and elasticity [112,113]. In recent years, advancements in DDS, such as nanocarriers, LCEs, and liposomes, have significantly enhanced the stability, skin penetration capability, and targeting efficiency of active ingredients, providing safer, more effective, and personalized strategies for skin rejuvenation [114].
3.
Natural active ingredients for skin health: Mechanisms and applications
The previous section discussed the causes and treatments of skin conditions such as immune imbalance, gland disorders, and chronic wounds. This section builds on that by highlighting key natural active ingredients, grouped by their main functions: anti-inflammatory and antioxidant effects, pigmentation control, hydration and skin barrier repair, and anti-aging benefits.
Rather than targeting a single disease, this section emphasizes the broad therapeutic roles of natural compounds across various skin conditions. Plant-derived agents such as resveratrol, baicalein, chlorogenic acid, and quercetin contribute to skin repair and protection by modulating key molecular pathways. Compared to synthetic substances, they offer better safety, skin compatibility, and multi-target effects. As the demand for safer and more sustainable skincare grows, these bioactive compounds are gaining increasing attention in formulations designed to support and restore skin health.
3.1
Antioxidant and anti-inflammatory mechanisms
Natural bioactive compounds play key roles in reducing skin inflammation and oxidative stress. Some act as free radical scavengers and inhibit lipid peroxidation, while others modulate immune responses and suppress inflammatory mediators, maintaining skin balance. Based on an extensive literature review, I believe that the multifactorial nature of skin inflammation supports combining bioactives with complementary mechanisms, such as flavonoids that regulate inflammation and antioxidants that counter oxidative stress, which may enhance efficacy and reduce both dosage and side effects.
Beyond basic skincare, many of these compounds also show therapeutic potential for inflammatory skin diseases such as AD, psoriasis, and acne. Polyphenols and flavonoids, for example, regulate key signaling pathways like NF-κB and MAPK, aiding in inflammation control [115,116]. Terpenoids, such as curcumin, inhibit cyclooxygenase-2 (COX-2) and reduce IL-6 and IL-1β levels, thereby alleviating symptoms of AD and psoriasis [117,118]. Phenolic acids, such as chlorogenic acid has demonstrated efficacy in psoriasis models by targeting the IL-17/IL-23 axis and improving barrier function [119]. Resveratrol reduces sebum production and suppresses C. acnes-induced inflammation, making it suitable for acne management. These natural compounds can be broadly classified into vitamins, polyphenols, carotenoids, flavonoids, essential oils, terpenoids, steroids, fatty acids, and plant extracts (Table S1 in Supporting information) [120-123].
3.2
Whitening mechanisms and pigmentation regulation
Pigmented skin disorders like melasma, freckles, and age spots are often linked to inflammation, oxidative stress, or hormone imbalance. These conditions not only affect appearance but can also damage the skin barrier or, in some cases, suggest a risk of cancer. Therefore, regulating melanin synthesis and distribution is important for both cosmetic and therapeutic reasons. Natural active compounds have shown potential in pigmentation management by inhibiting melanin production, enhancing its degradation, or blocking its transfer to keratinocytes. Their efficacy, however, also depends on individual skin conditions. For example, antioxidants such as VC and its derivatives are more effective against UV-induced pigmentation, whereas tyrosinase inhibitors like arbutin are preferable for other hyperpigmentation types.
As summarized in Table S2 (Supporting information), plant-derived ingredients can act on multiple targets within the melanogenic pathway. For example, arbutin and tretinoin are tyrosinase inhibitors that suppress melanin synthesis directly [124], while VC, its derivatives, and polyphenols reduce oxidative stress, which indirectly modulates melanocyte activity [125,126]. Anti-inflammatory agents like glycyrrhizic acid and aloe vera extract help control inflammation-induced hyperpigmentation by downregulating melanocyte activation [127,128]. Additionally, compounds such as salicylic acid and fruit acids promote epidermal turnover and melanin removal [129], while nicotinamide and VC derivatives inhibit melanin transport from melanocytes to keratinocytes [130]. Some ingredients, including myostatin inhibitors and extracts, may also counteract glycation-induced skin yellowing by inhibiting the formation of AGEs [131,132]. These multifaceted mechanisms highlight the value of natural actives not only for improving skin tone but also for managing pigmentation-related skin conditions.
3.3
Hydration, sebum regulation, and barrier protection
Disruption of the skin's moisture-oil balance is closely linked to dermatological conditions such as seborrheic dermatitis and acne. Excess sebum production, often coupled with compromised skin barrier function, can lead to inflammation, clogged pores, and microbial overgrowth. Therefore, restoring hydration, regulating sebum secretion, and reinforcing the skin's barrier are essential strategies in both skincare and the prevention or alleviation of these conditions.
Several natural compounds contribute to these functions through targeted biological mechanisms, as summarized in Table S3 (Supporting information). For instance, polysaccharides in Aloe vera retain moisture, modulate sebaceous gland activity, and exert anti-inflammatory effects, making them beneficial for oily and irritated skin [133]. Tea tree oil, known for its antibacterial and anti-inflammatory properties, not only helps control sebum but also reduces acne lesions without excessively drying the skin [134]. Jojoba oil, due to its structural similarity to human sebum, penetrates deeply to maintain hydration while regulating oil secretion and preventing pore blockage [135,136]. Additionally, aloe vera, rose water and cucumber extract, rich in hydration and natural astringents, help soothe inflamed skin, tighten enlarged pores, and limit sebum overproduction [137,138]. However, the effectiveness of these ingredients is not solely determined by the active compounds but also by factors such as skin type, usage conditions, and external factors. For instance, while jojoba oil can deeply penetrate the skin and regulate sebum secretion, it may feel greasy for individuals with already oily skin, leading to less favorable user experiences. Thus, when selecting natural ingredients, it is crucial to consider individual skin conditions and care goals to optimize results.
3.4
Anti-aging mechanisms and treatment for skin disorders
Aging-related skin disorders, such as dry dermatitis, wrinkles, discoloration, sagging skin, and inflammatory conditions like eczema and psoriasis, are common concerns for many individuals. These conditions are often exacerbated by factors such as aging, sun exposure, and lifestyle choices. Delaying skin aging and addressing these aging-related skin disorders requires a multifaceted approach that includes reducing oxidative stress [139], controlling inflammation, inhibiting protein glycation, and modulating gene expression associated with aging.
Natural active ingredients play a pivotal role in this process. They have been shown to slow down skin aging by promoting cellular regeneration, stimulating collagen synthesis, and enhancing skin elasticity and firmness [140-142]. In addition to these anti-aging effects, certain natural compounds also demonstrate therapeutic potential for treating age-related skin conditions such as chronic dryness, eczema, and psoriasis. For example, compounds like resveratrol, baicalein, and certain flavonoids possess anti-inflammatory and antioxidative properties that not only help to rejuvenate the skin but also alleviate inflammation and skin irritation associated with conditions like eczema and psoriasis [143]. Therefore, future studies should focus more on the delivery efficiency of these compounds in different skin aging models, as well as their interactions with the skin microbiome.
4.
Topical skin DDS for the delivery of natural active substances
Although many natural active compounds show great potential for treating skin diseases and skin care, their physicochemical properties often limit their effectiveness. Many insoluble natural actives are difficult to deliver efficiently with conventional formulations. Furthermore, most topical products have limited penetration beyond the stratum corneum and do not reach systemic circulation, acting mainly on the skin surface. This poses a challenge for treatments requiring deeper skin layer penetration [144]. DDS refers to the process of delivering therapeutic drugs through various forms of administration for disease prevention and treatment. The development of nano-delivery systems has provided effective solutions for the dermal delivery of natural active products. Various nano-delivery systems are now being used to deliver these natural actives for the treatment of skin diseases and skin care, as summarized in Table S4 (Supporting information).
4.1
Nanocarrier systems
4.1.1
NEs
NEs are stable colloidal dispersion systems, formed by dispersing emulsion droplets with a particle size ranging from 20 nanometers to 200 nanometers in another liquid phase [145]. Based on their structural characteristics, NEs can be classified into water-in-oil (W/O), oil-in-water (O/W), and double continuous (O/W/O or W/O/W) systems [146]. Due to their unique structure and properties, NEs are widely studied for delivering active substances because of their special structure and properties. They improve skin penetration in several ways. First, they can dissolve both water- and fat-soluble drugs, allowing for higher drug loading and flexible dosing. Second, their structure helps the emulsion particles stick closely to the skin, improving contact with the stratum corneum. Third, the oil and surfactants can disrupt the skin's lipid layers to boost absorption, while the water phase keeps the skin hydrated, making it easier for drugs to pass through [147-150].
The advantages of NEs in skin treatment lie primarily in their exceptional local drug delivery and skin penetration properties. Their high surface area, small particle size, and unique oil-water interactions enable drugs to effectively penetrate both the skin surface and deeper layers, NEs can carry natural active substances and penetrate the skin surface effectively. In a study by Giacone et al. [151], the use of drug-loaded NEs for local administration in two-dimensional and three-dimensional skin cancer models demonstrated that chitosan NEs with oleic acid significantly enhanced the permeability of drugs and other molecules in the skin. The absolute amount of drug in the skin increased by approximately 15 times, indicating the system's stronger local drug delivery capacity. In another application, Pleguezuelos-Villa et al. [152] prepared hyaluronic acid NEs, which improved their adhesion and stability to the skin, enhancing the bioavailability of mangiferin and resulting in better efficacy in anti-inflammatory and antioxidant treatments. These studies provide new insights into the application of NEs in the treatment of skin diseases.
The delivery properties of NEs make them highly promising in skin treatments, particularly excelling in antioxidant and anti-inflammatory applications [153]. In antioxidant therapy, NEs can effectively deliver antioxidants, such as VC, VE, and coenzyme Q10, to the skin to neutralize free radicals, significantly reducing oxidative damage caused by UV radiation and environmental pollution [154,155]. For example, Butnariu et al. [156] explored the use of propolis aqueous solution and lycopene extract NEs in protecting the skin from UVA radiation. This nan emulsion achieved controlled local release, extended the duration of the extract's action, and enhanced the skin's absorption. The antioxidant and anti-inflammatory effects of lycopene were amplified, and the nan emulsion also promoted the regeneration of skin affected by fungal or microbial infections. Alzorqi et al. [157] incorporated β-d-glucan into a palm oil-based nan emulsion as a carrier system for skin care and treatment. The study optimized the ultrasound-induced emulsification method to reduce the droplet diameter and viscosity, thereby enhancing the delivery of β-d-glucan while maximizing the antioxidant load and stability of the emulsion. In anti-inflammatory treatments, Borges et al. [158] studied NEs optimized for the oil phase and found that they effectively delivered anti-inflammatory agents, such as dapsone, deep into the skin, increasing local concentrations and quickly alleviating inflammation caused by excessive sebum secretion or external stimuli, such as redness and acne. To provide sustained drug release on the skin surface and enable multiple mechanisms to collaboratively treat diseases, Chamchangi et al. [159] combined nan hydrogels with NEs. Their study revealed that increasing the proportion of nan emulsion significantly enhanced anti-inflammatory properties, promoted tissue repair, and increased epidermal thickness. The biphasic structure of NEs (water and oil phases) helps increase hydration in the stratum corneum, improving skin barrier function and reducing the likelihood of inflammation [160-162]. Due to their dual advantages of antioxidant and anti-inflammatory effects, NEs hold vast potential for applications, especially in treating acne, sensitive skin, and aging skin.
Many studies have shown that nanoemulsions (NEs) have clear advantages over traditional formulations. They improve absorption, enhance stability, and extend the effect of active ingredients. Their biphasic structure allows both water- and oil-soluble ingredients to be combined, making them suitable for multifunctional skincare. As a result, NEs are seen as a promising option for treating skin problems like acne, photoaging, and inflammation.
4.1.2
Nanocrystals
Nanocrystals are pure drug crystals sized 10–1000 nm. Their ultrafine dimensions and high drug loading enable superior skin penetration and bioavailability compared with conventional topical formulations, thereby enhancing therapeutic efficacy [163-165]. For example, curcumin's poor skin permeability is overcome by formulating it as nanocrystals: fluorescence imaging shows these particles reach deeper dermal layers, and when embedded in a moisturizing hydrogel, they achieve high follicular targeting and drug deposition [166,167].
Reduction in particle size leads to increased apparent solubility, thereby generating a steeper concentration gradient that facilitates passive diffusion across the skin barrier [168-170]. Moreover, surface functionalization enhances interactions with skin constituents, further improving permeation efficiency [171]. Nanocrystals can significantly enhance drug solubility and bioavailability by decreasing particle size, increasing surface area, and employing optimized delivery formulations. Clinically, nanocrystal-based systems have accelerated wound healing and reduced inflammation. In a postoperative tumor model with bacterial infection, a bioactive glass-ceramic nanodrug achieved faster wound closure and minimal inflammation compared with controls [172]. A bacterial-cellulose/gelatin hydrogel containing selenium nanocrystals promoted full-thickness skin regeneration in rats by elevating ROS to kill bacteria and stimulate tissue repair [173]. Topical nanosilver effectively alleviated DNFB-induced contact dermatitis in mice, reducing edema and inflammatory cell infiltration more broadly than tacrolimus or steroids [174]. Nanocrystal technology has great academic and practical value for delivering natural active compounds through the skin. It can improve the delivery of poorly soluble drugs by offering high drug loading and good skin penetration. Surface modifications also help target specific areas like hair follicles or inflamed skin, making treatment more precise [175].
4.1.3
Liposomes
Liposomes, as a prominent DDS for topical applications, are composed of lipid bilayers mimicking cellular membranes, including both conventional forms and various modified variants [176]. This unique structure endows them with excellent skin affinity and biocompatibility, effectively reducing irritation and making them suitable for long-term use [177]. Liposomes not only offer good stability but also improve drug absorption and skin penetration, as shown in Fig. S5 (Supporting information), their surface can be adjusted to target delivery, raise local drug levels, and enhance treatment effects (Fig. S5A). They can carry both water- and fat-soluble drugs, and allow controlled release by changing bilayer fluidity or adding surface functions, helping to prolong effects and reduce use frequency [177,178]. Given their membrane-mimicking structure and skin compatibility, liposomes offer notable advantages in delivering natural active ingredients through the skin. By adjusting particle size, surface charge, and chemical modifications, they can also achieve targeted delivery to specific skin regions such as hair follicles or inflammatory sites, enhancing treatment precision and safety.
In terms of permeability and stability, liposomes outperform many other nanocarriers. Their flexible bilayer structure facilitates the penetration of active compounds across the stratum corneum, allowing them to reach the epidermis and even the dermis [179]. They are also capable of stabilizing sensitive natural ingredients such as antioxidants and vitamins, preventing degradation due to light or oxidation [180]. Additionally, liposomes exhibit high drug-loading efficiency and enable sustained drug release, thereby prolonging residence time on the skin and reducing the frequency of use [181]. Surface modifications, such as tuning particle size and charge, further enhance their targeting capabilities to inflamed tissues or hair follicles (Fig. S5B), boosting local therapeutic effects [182]. Their permeation mechanisms include hydration, penetration, and fusion, which disrupt the stratum corneum structure and increase skin hydration, thereby facilitating drug diffusion and absorption [183-185].
Liposomes also demonstrate considerable potential in skin whitening and melanoma therapy. Studies have shown that liposomes can selectively target melanocytes, suppress melanin production and transport, and extend the duration of whitening agents on the skin, thereby enhancing their efficacy [186]. For instance, arbutin-loaded liposomes exhibit significantly greater deposition in the epidermis and dermis compared to aqueous solutions, markedly improving the skin bioavailability of hydrophilic agents [187]. As shown in Figs. S5C and D, liposomes carrying natural active ingredients show strong therapeutic effects in melanoma models. After light activation, the neutral liposomes become positively charged, helping them stick to blood vessels and enter cells more easily. This suggests they are useful for delivering drugs deep into the skin. Future studies should focus on creating smart liposomes that combine controlled release, targeted delivery, and better skin penetration to support the clinical use of natural compounds in skin treatments and skincare.
4.1.4
Solid lipid nanoparticles
Among solid particulate delivery systems, nanoparticles represent a widely used and well-studied category. Nanoparticles, defined as solid particles ranging in size from 1 nm to 100 nm, possess distinctive physicochemical properties such as a high surface area-to-volume ratio, excellent stability, and tunable surface functionalities. Due to their diverse morphology, size, surface charge, and modifiability, nanoparticles have found broad applications in topical formulations, particularly in the treatment of skin diseases, anti-aging therapies, and functional skincare [188,189]. Their nanoscale dimensions enable them to penetrate the skin via intercellular spaces in the stratum corneum or appendages such as hair follicles, thereby enhancing the permeability and bioavailability of active ingredients. Key factors influencing their skin penetration include particle size, shape, surface charge, drug loading capacity, and encapsulation efficiency. Notably, particles smaller than 100 nm and positively charged nanoparticles exhibit superior skin permeability [190-193].
Functionalized nanoparticles further improve therapeutic efficacy and delivery precision. For instance, chitosan-modified nanoparticles (CSNPs) enhance drug accumulation in deeper skin layers, facilitate sustained release, and reduce drug loss [194]. Additionally, by adjusting material composition and surface modification, the drug release profile can be finely controlled, which is particularly beneficial for delivering environment-sensitive agents such as proteins [195,196]. Huang et al. demonstrated that gold nanoparticles (Au-NPs) could enhance the skin permeability and facilitate the delivery of large hydrophilic protein drugs, bypassing complex loading processes while preserving the bioactivity of both drugs and carriers [197,198].
Nanoparticles have also shown promising potential in the treatment of skin disorders. In the case of AD, co-loading hydroxytyrosol (HT), a potent antioxidant, with hydrocortisone (HC) into a nanoparticle system significantly improved symptoms such as erythema, inflammation, and TEWL, achieving better outcomes compared to conventional treatments [199]. In psoriasis models, cationic nanoparticles (cNPs) were able to competitively bind to DNA in DNA-LL37 immune complexes, effectively suppressing aberrant immune activation. Phenotypic imaging, histological analysis, and animal studies confirmed that topical application of cNPs alleviated inflammation with high skin retention and low systemic toxicity [200].
Beyond therapeutic use, nanoparticles are extensively incorporated into sunscreen and whitening products. Inorganic nanoparticles such as titanium dioxide (TiO2) and zinc oxide (ZnO) are widely utilized in physical sunscreens due to their ability to block UV radiation without causing irritation or allergic reactions [201]. To address the safety concerns of organic UV filters penetrating the skin and disrupting hormonal balance, researchers have developed bioadhesive polymeric nanoparticles (BNPs) that encapsulate the active ingredients and retain them on the skin surface, preventing follicular penetration while maintaining effective photoprotection at low concentrations [202]. Moreover, dual-functional nanomaterials such as TiO2/ZnO microspheres have been designed to minimize visible light reflection, reduce whitening effects, and enhance product aesthetics and safety, advantages that conventional materials fail to offer [203].
4.1.5
Polymeric micelles
Polymeric micelles are nanoscale structures formed by the self-assembly of polymeric molecules, which have both hydrophilic and hydrophobic regions, enabling them to maintain stability in aqueous environments [204]. This self-assembly process is driven by hydrophobic interactions between polymeric chains, and factors such as chain length, structure, hydrophilic-to-hydrophobic ratio, and polymeric concentration influence their stability and morphology. Polymeric micelles have widespread applications in drug delivery, gene transport, and nanomaterial development. By interacting with skin lipids, they enhance drug permeability and moisturizing effects, improving the ability of active ingredients to penetrate deeper into the skin.
In topical formulations, polymeric micelles deliver drugs well by improving permeability, targeting locally, controlling release, reducing irritation, and enhancing stability. Their skin penetration depends on several factors: the polymer's molecular weight, chain length, shape, and hydrophilic-hydrophobic balance affect micelle formation and stability. Meanwhile, drug solubility, formulation ingredients, and external conditions also impact how well they penetrate. For example, the GQA polymer's mild positive charge and medium molecular weight mPEG help optimize micelle surface properties [205], while hydrophobic drugs (such as indomethacin and resveratrol) in PEG-amino acid micelles exhibit higher solubility and sustained release, further enhancing skin penetration and efficacy [206]. External factors, such as temperature and the duration of the formulation's stay on the skin, significantly influence drug release behavior [207].
Polymeric micelles are particularly prominent in anti-aging skincare products because they can effectively enhance the stability and permeability of active ingredients, directly addressing the root causes of aging, such as free radical damage and collagen loss. For example, Seo et al. [208] combined gold nanoparticles with polyaspartic acid-based polymeric micelles, which facilitated the cellular uptake and delivery of VC; Channarong et al. [209] developed a polymer mixed micelle that significantly improved the stability and antioxidant activity of curcumin, further demonstrating the potential of polymeric micelles in delivering natural active ingredients.
4.2
Structured emulsion-based systems
LCEs and Pickering emulsions are two rapidly advancing formulation systems that are frequently categorized as nanodelivery systems. This classification is primarily attributed to their nanoscale structural characteristics and their significant enhancement of active ingredient delivery efficiency. LCEs exhibit nanoscale, orderly arranged structures formed through interactions between surfactants and the oil-water phases, thereby improving the stability of natural bioactives and enabling controlled release. In contrast, Pickering emulsions are stabilized by solid particles at the oil–water interface, forming highly stable emulsions. These particles typically range in size from the nanometer to submicron scale, allowing for improved skin adhesion and permeability without the use of surfactants. Due to their structural features and delivery performance, both types of emulsions are widely recognized as part of topical nanosystems and have demonstrated great potential in functional skincare and the treatment of dermatological conditions.
4.2.1
LCEs
LCEs are an intermediate-phase system that combines the ordered structure of crystals with the fluidity of liquids. They are widely applied in topical drug delivery and skincare products [210]. The lamellar LC structure they form closely mimics the lipid arrangement of the skin's stratum corneum, enhancing the compatibility of the formulation with the skin and improving the stability and penetration efficiency of active ingredients [211]. Compared to traditional emulsions, LC structures offer superior controlled release properties, moisturizing effects, and user experience, effectively addressing issues such as dry and damaged skin barriers [212]. Fig. S6 (Supporting information) illustrates the crystallization process (Fig. S6A) and structure (Fig. S6B) of the drug in a LCEs, observable under polarized light microscopy [213].
The delivery advantages of LCEs stem primarily from their stable structure and excellent biocompatibility. On one hand, the ordered arrangement of LC molecules significantly enhances the stability of the system, enabling effective encapsulation and protection of unstable components such as VC [214,215]. On the other hand, the small and uniform droplet structure of the LC emulsion increases the contact area with the skin, facilitating the penetration and absorption of active ingredients. Eva María Arias et al. found that although micellar solutions can enhance skin permeation by increasing skin hydration, their effectiveness in controlled drug release and skin accumulation is limited. In contrast, liquid crystal emulsions with a higher proportion of LC structures significantly improve drug penetration through the stratum corneum and enhance retention in both the epidermis and dermis, demonstrating superior transdermal delivery efficiency. Therefore, LC structures offer distinct advantages in promoting drug delivery through the skin [216]. Additionally, the LC structure effectively locks in moisture, reducing water evaporation, providing significant moisturizing and soothing effects, especially beneficial for dry and sensitive skin [217], while minimizing the irritation to active ingredients, which helps reduce the risk of inflammation [218].
The skin penetration behavior of LCEs is influenced by several factors, including the type and concentration of surfactants, preparation temperature, and the type of LC phase. High-ordered cubic and hexagonal LC phases serve as ideal matrices for controlled drug release, promoting the penetration of drug molecules through the skin barrier [219]. Increased LC content also enhances skin hydration, further improving the absorption efficiency of active ingredients [220]. Currently, LCEs demonstrate excellent performance in various skincare products. For example, Perrier's patented LC cream forms a biomimetic moisturizing film on the skin's surface, while Rare Collection's Matsutake LC cream provides oil control, soothing, and repair effects, making it particularly suitable for daily care of sensitive skin. The effects of these products are shown in Fig. S6C, further showcasing the potential of LCEs in biological drug delivery applications.
4.2.2
Pickering emulsions
Pickering emulsions are a type of emulsion stabilized by solid particles such as starch nanoparticles, polysaccharides, or titanium dioxide, unlike traditional emulsions that rely on surfactants. Instead, these emulsions achieve stability by adsorbing particles onto the surfaces of oil droplets [221]. As shown in Fig. S7 (Supporting information), the emulsion is most stable when the contact angle of the particles with both the oil and water phases is close to 90° (Fig. S7A) [222].
This unique stabilization mechanism gives Pickering emulsions significant advantages, including environmental friendliness, biocompatibility, and high stability [223]. In addition to their high stability and low environmental impact, Pickering emulsions enhance the skin penetration delivery of active ingredients, particularly improving penetration through the stratum corneum, without the need for additional permeation enhancers (Fig. S7B) [224]. Furthermore, Pickering emulsions outperform traditional emulsions in thermodynamic stability. For example, emulsions stabilized by modified silica nanoparticles can remain stable at room temperature for up to three months, whereas conventional emulsions typically last only about a month [225,226].
Pickering emulsions hold great potential in skin care, particularly in drug delivery. The small particle size allows them to better penetrate the skin barrier while offering superior biocompatibility [224]. Their controlled release properties make them ideal carriers for topical medications, extending the therapeutic duration and reducing the discomfort or irritation associated with drug bursts [227]. Moreover, factors such as the polarity and fatty acid structure of the oil phase, particle wettability, size, and concentration all significantly influence the permeability and stability of the emulsion [228,229]. Therefore, precise control of these factors during preparation is essential to ensure optimal skin penetration and therapeutic efficacy. Fig. S7C demonstrates how Pickering emulsions exhibit improved stability and permeability at specific pH values.
These characteristics make Pickering emulsions particularly suitable for sensitive skin care, especially in the application of anti-aging and antioxidant products. Due to their excellent permeability, Pickering emulsions can efficiently deliver natural active ingredients such as antioxidants, VC, and flavonoids [230,231]. For instance, studies have shown that Pickering emulsions containing tocopheryl acetate (TA) effectively neutralize free radicals, delay the aging process, and enhance UV stability, with minimal cytotoxicity on skin cells. This results in clear anti-aging effects [232]. These attributes position Pickering emulsions as a promising delivery system in both skin care and pharmaceutical applications.
4.3
Other advanced delivery systems
4.3.1
EXOs
EXOs are nanosized vesicles, typically 40–100 nanometers in diameter, secreted by eukaryotic cells. They carry active biomolecules identical to those of their parent cells and play a crucial role in intercellular communication. EXOs can transport lipids, proteins, polysaccharides, and nucleic acids, thereby facilitating the exchange of genetic information [233]. Their biological functions are primarily mediated through two mechanisms: first, the surface molecules of EXOs bind to receptors on target cells, activating intracellular signaling pathways; second, EXOs can be internalized by target cells, delivering their genetic content to regulate cellular activities. In the field of skincare, EXOs can be absorbed by various skin cells, such as keratinocytes, fibroblasts, immune cells, and endothelial cells, contributing to improved skin health by promoting wound healing, enhancing vascularization, modulating inflammatory responses, and recruiting stem cells [234].
In drug delivery, EXOs exhibit remarkable advantages due to their excellent biocompatibility and ability to enhance skin permeability. With diameters ranging from 30 nm to 200 nm, EXOs can easily traverse the skin barrier, enabling efficient release of active compounds and therapeutic effects [235]. Particularly, MSCs-derived EXOs demonstrate superior drug-loading capacity and targeting ability, significantly enhancing drug efficacy while minimizing side effects [236]. Additionally, the growth factors and cytokines carried by EXOs stimulate skin cell proliferation and migration, accelerating wound healing [237]. EXOs also exhibit anti-inflammatory, antioxidant, and immunomodulatory properties. For instance, MSC-derived EXOs can activate the Nrf2/Keap1 pathway to alleviate oxidative stress and repair skin damage caused by aging or UV exposure [238]. Factors such as EXO size, skin condition, and surface modification techniques can significantly influence their percutaneous penetration and targeting efficiency [239,240].
As natural carriers for intercellular communication, EXOs show great promise in anti-aging and tissue regeneration applications due to their outstanding biocompatibility and permeability. They can effectively deliver active molecules, including proteins, RNA, cytokines, and growth factors, to stimulate collagen production, reduce inflammation, and promote skin renewal and repair, thereby slowing down the aging process. Leading skincare brands such as Angela Caglia have adopted EXO-based technologies in their premium products to improve skin elasticity and smoothness [241,242]. Studies have demonstrated that EXOs not only accelerate tissue regeneration but also hold therapeutic potential for hair loss by promoting hair follicle regeneration and delaying follicular aging, offering innovative solutions for both anti-aging skincare and hair restoration [243,244].
4.3.2
Microcapsules
Microcapsules are an emerging DDS that encapsulate active ingredients within a capsule wall, with particle sizes typically ranging from 5 μm to 300 μm [245]. These microcapsules can be classified into various structural types, including mononuclear, multinuclear, and bilayer structures [246]. One of their primary advantages is the ability to provide a stable internal environment for natural active compounds, effectively preventing adverse reactions with the external environment and shielding sensitive ingredients from degradation. This feature renders microcapsules particularly suitable for incorporating unstable natural compounds into topical skincare products, addressing challenges such as volatility and high reactivity [247].
In practical applications, microcapsules have been widely used to improve the stability and efficacy of topical formulations by encapsulating natural extracts, antioxidants, and moisturizing agents [248,249]. For instance, patented microencapsulation techniques have been employed in loose powders to incorporate botanical ingredients such as Perilla and Amaranth, preserving their bioactivity and enhancing product stability [250]. Similarly, this technology has been employed in rinse-off formulations, where Fechii applied microencapsulation to reduce the volatility of natural active ingredients and enhance their stability, thereby extending their effects on the skin and improving the overall user experience [251]. Furthermore, by adjusting the carrier composition, structure, size, and processing conditions, microcapsules can achieve controlled drug release, thereby prolonging the activity of active ingredients and reducing toxicity and volatility [252]. Studies have confirmed that cumulative release of thymol (THY) from cellulose acetate microcapsules and sustained release from microcapsules improves efficacy and minimizes adverse effects [253]. Moreover, microcapsules isolate active compounds from external agents, preventing oxidation or chemical degradation. The release profile can be fine-tuned by modifying shell thickness, optimizing stability to meet specific therapeutic goals [254]. Microencapsulation also allows for the uniform incorporation of otherwise incompatible ingredients [255]. Zhang et al. [256] demonstrated that encapsulating UV absorbers within microcapsules effectively prevents photodegradation and adverse interactions, thereby improving the safety and stability of sunscreen formulations.
Microencapsulation technology primarily targets the epidermis and stratum corneum, where the capsules adhere to the skin surface and gradually release active compounds, providing long-lasting effects [257,258]. It offers notable benefits in regulating the skin's oil-water balance. For example, microcapsules containing oil-absorbing powders or botanical extracts can slowly release sebum-controlling agents upon rupture, effectively reducing excess oil [259]. Meanwhile, encapsulated moisturizing agents such as hyaluronic acid and glycerin deliver prolonged hydration by releasing water gradually into the skin [260]. This precise release mechanism enables a balanced oil-water ratio on the skin's surface, avoiding both dryness and excessive greasiness. Consequently, microcapsules are particularly well-suited for oily and combination skin types, addressing dual concerns of dehydration and shine with one delivery system.
4.3.3
Other innovative systems
The domestic definition of topical skin products is quite broad, encompassing products that are applied to human skin, hair, nails, lips, and other body parts through methods such as application, sprinkling, or spraying. These products are designed for various purposes, including cleansing, fragrancing, altering appearance, correcting odors, or maintaining skin health. As a result, the market includes not only products based on novel delivery technologies, but also many products that are classified according to other criteria, such as their specific functions (e.g., moisturizers, sunscreens, anti-aging treatments) or target skin conditions (e.g., acne, dermatitis, pigmentation).
With the continuous development of new products and technologies, not only are surface skincare formulations being optimized, but medical aesthetic devices are also gradually entering the market. As shown in Fig. S8 (Supporting information), hydration injection is one such injectable cosmetic treatment used to enhance skin health, with its therapeutic effects illustrated in Fig. S8A. Hydration injections use negative pressure to deliver active ingredients directly into the dermis. They often contain small molecules of sodium hyaluronate, which are highly water-binding. With ultra-micro-penetration technology, these injections quickly hydrate the deeper skin layers. Studies show that combining IPL with hyaluronic acid hydrafacial injections is more effective for treating melasma than hydroxydermabrasion alone. This combination reduces TEWL and melasma severity scores, showing better skin barrier repair. Side effects were similar between the two treatments, suggesting that IPL enhances the overall effect. This combined method is both effective and practical for melasma care [261].
Microneedling (MN) is a procedure that involves using tiny needles to create micro-wounds in the skin. These micro-punctures trigger the skin's natural healing process, stimulating the production of collagen and elastin. The process is depicted in Fig. S8B. As the pinholes are created, certain natural skincare substances (e.g., polyphenols, hyaluronic acid) can penetrate more effectively into the deeper layers of the skin through these micro-channels, thereby enhancing the therapeutic effects on the skin. There are two types of MN: superficial and deep. Superficial MN (0.25–0.5 mm) primarily targets the epidermis to enhance the absorption of skincare products and improve skin tone. In contrast, deep MN (1–2 mm) reaches the dermis and is suitable for treating more serious skin issues such as acne scars, folliculitis, and wrinkles [262].
Radio frequency (RF) technology is an advanced medical cosmetology technique that uses specific electromagnetic waves to directly target the dermis layer of the skin. It offers improved therapeutic effects and a broader range of applications, as shown in Fig. S8C. Similar to hydration injections, RF technology has hydrating and moisturising benefits, but it also goes a step further by adjusting and activating melanin and aged cells in the skin through electromagnetic waves. This leads to a range of skin benefits, including anti-wrinkle effects, lightening of hyperpigmentation, pore reduction, and skin tightening. One of the key advantages of RF treatments is their minimal side effects. The results from RF therapy can last between 1 year to 2 years, significantly reducing the frequency of treatments required and improving patient compliance [263].
5.
Summary
Natural active ingredients are increasingly favored in topical skin preparations due to their low side effects and multiple biological activities, including anti-inflammatory, antioxidant, antimicrobial, and moisturizing properties [264]. However, natural ingredients often have problems like poor skin absorption, low stability, and easy breakdown during storage or use. The skin's barrier also makes it hard for them to reach deeper layers, reducing their effectiveness. In addition, people's skin reacts differently, so the same delivery method may not work equally for everyone. To solve these issues, researchers are focusing on new delivery systems that improve ingredient stability and help them better reach target areas in the skin. This is now a major focus in topical drug delivery research [265].
Currently, researchers are now developing multifunctional carriers like nanostructures that can promote absorption, release drugs slowly, and target specific areas. These systems help keep natural ingredients stable and control their release in the skin, making treatments more effective [266]. Simultaneously, new natural materials like polysaccharides and proteins have been developed. They are biocompatible and can work with natural extracts to improve the skin absorption of active ingredients, making the products more effective and safer [267]. With biotech advances, smart and personalized DDS are emerging, allowing more precise treatment by adjusting the release of active ingredients based on skin conditions. This shows great promise for future skin care and therapy [268].
As research into natural active ingredient delivery systems continues to advance, significant progress has been made with innovative methods such as nanotechnology, microneedle technology, and biomaterials [269]. However, key challenges remain, such as improving skin permeability, enhancing stability, and overcoming the skin barrier. The reasons behind different individual responses to natural ingredients are still unclear, and creating personalized treatments based on skin type, age, and health is an important goal. Future research should focus more on developing "multifunctional" and "smart" delivery systems, which will need both new technologies and teamwork across different fields. As precision medicine advances, customizing delivery systems based on skin conditions and personal features will help improve treatment results and patient compliance. In addition, using big data and AI can allow real-time skin monitoring and adjust delivery strategies accordingly. This is expected to be a major future trend. Studying topical delivery of natural ingredients not only supports better skincare and treatment but also brings new opportunities for personalized and intelligent dermatology. Continued innovation in this area will help create safer and more effective treatments and promote healthier skin.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figure 1
(A) Structure of the skin, including the epidermis, dermis (papillary and reticular layers), and hypodermis, with key adnexal structures indicated. Copied with permission [3]. Copyright 2015, American Society for Clinical Investigation. (B) Schematic diagram of the pathway of drug penetration through the skin. Reproduced with permission [6]. Copyright 2011, Elsevier.

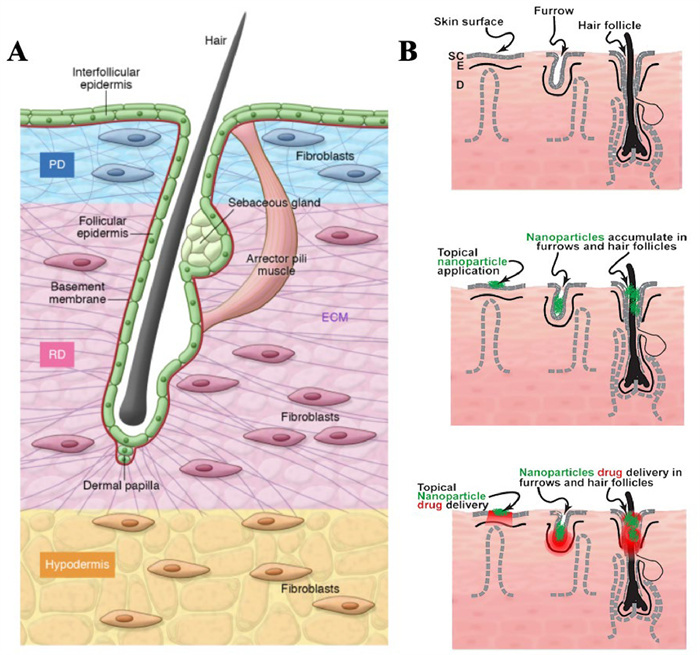
 DownLoad:
DownLoad:
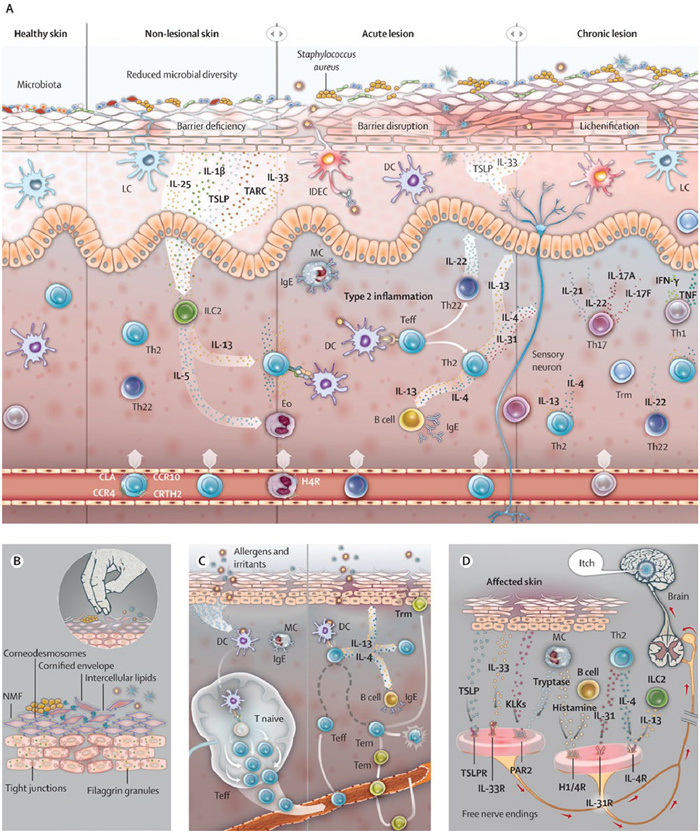

 下载:
下载:



 下载:
下载:
