Figure 1.
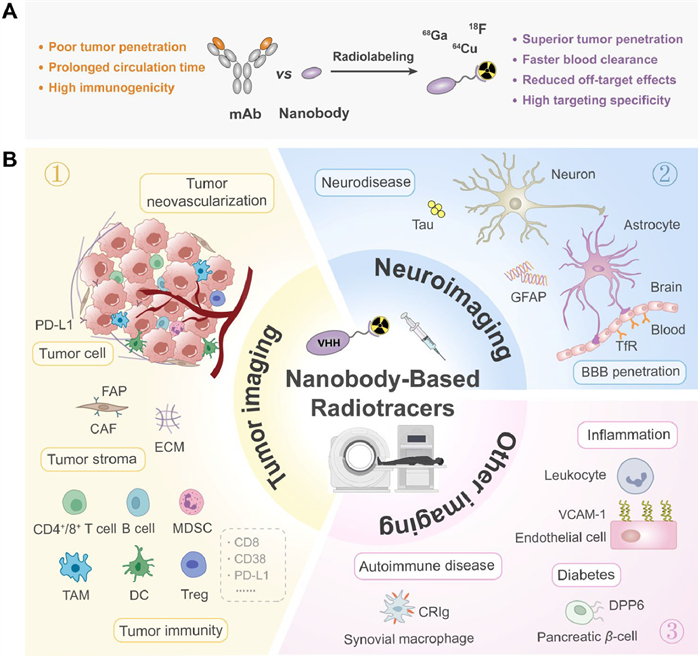
(A) Key advantages of nanobody-based radiotracers. (B) Overview of targets for nanobody-based radiotracers in nuclear medicine.
Nanobody-based radiotracers in nuclear medicine: Advances, challenges, and future perspectives
Ying Yao , Juan Tian , Ran Zhang , Ping Liu , Xiang Gao , Wenhu Zhou , Longlong Luo

Accurate and early disease diagnosis is critical for improving patient survival and guiding therapeutic decisions [1]. Nuclear medicine imaging, particularly positron emission tomography (PET) and single-photon emission computed tomography (SPECT), has revolutionized medical diagnostics by enabling real-time, non-invasive visualization of biological processes at the molecular level [2-4]. These techniques utilize radiopharmaceuticals that selectively bind to disease-specific biomarkers, providing high-resolution imaging for disease localization, staging, and treatment monitoring [5,6].
Conventional radiotracers, such as [18F]fluorodeoxyglucose ([18F]F-FDG), are widely used in PET imaging to assess glucose metabolism in tumors [7]. However, [18F]F-FDG lacks specificity, as inflammatory and infectious lesions also exhibit high uptake, leading to false-positive results [8-12]. To improve tumor specificity, targeted radiotracers, including monoclonal antibodies (mAbs), small molecules, and peptide-based probes, have been developed [13]. Despite these advancements, each class of radiotracers has inherent limitations: mAbs exhibit poor tumor penetration and prolonged circulation times [14]; small molecules often lack sufficient specificity and undergo rapid renal clearance [15]; and peptide-based tracers are prone to enzymatic degradation and display relatively low binding affinity [16]. These challenges continue to hinder the development of radiotracers with optimal imaging efficacy.
To overcome these limitations, nanobodies, also called single-domain antibodies (sdAbs) or heavy-chain variable domain antibodies (VHHs), have emerged as a promising platform in nuclear medicine imaging [14]. Nanobodies, the single-domain antigen-binding fragments derived from heavy-chain-only antibodies (HCAbs) of camelids, possess several advantages over conventional mAbs, including smaller molecular size (~15 kDa), enhanced tissue penetration, rapid systemic clearance, and reduced immunogenicity [17-21]. These properties make nanobodies particularly well-suited for molecular imaging and theranostic applications, where rapid targeting and minimal off-target effects are essential.
The integration of nanobody technology with radiopharmaceuticals has driven significant progress in PET and SPECT imaging. Recent advancements in nanobody engineering have led to the development of high-performance radiotracers targeting oncogenic biomarkers such as human epidermal growth factor receptor 2 (HER2), prostate-specific membrane antigen (PSMA), and programmed death-ligand 1 (PD-L1), facilitating early tumor detection and personalized treatment planning [22]. Beyond oncology, nanobody-based imaging has expanded into other disease areas, including neuroinflammation and immune system disorders, broadening the landscape of molecular diagnostics [23].
Despite these promising advancements, the clinical translation of nanobody-based radiopharmaceuticals still faces several challenges, including the optimization of radiolabeling strategies, reduction of renal retentio and prolongation of circulation half-life to meet therapeutic demands. Additionally, the integration of artificial intelligence (AI) is expected to revolutionize the field by accelerating the discovery, optimization, and radiolabeling of nanobody-based tracers, ultimately enhancing imaging accuracy and therapeutic efficacy.
This review provides a comprehensive analysis of the latest developments in nanobody-based radiotracers for nuclear medicine imaging. As the field continues to evolve, nanobody-based radiopharmaceuticals are expected to play a central role in advancing nuclear medicine, ultimately improving diagnostic accuracy, therapeutic efficacy, and patient outcomes across multiple disease domains (Fig. 1).
Since their discovery in the early 1990s [24], nanobodies have garnered significant attention as a promising alternative to conventional mAbs due to their small molecular size (~12–15 kDa), high stability, and remarkable target specificity [25]. Unlike conventional antibodies, which are composed of two heavy and two light chains, nanobodies lack light chains and possess a single variable domain that mediates antigen recognition (Fig. S1 in Supporting information) [26]. Their unique advantages arise from several key structural and biochemical characteristics, as outlined below.
(1) High affinity and broad epitope recognition: Nanobodies possess high antigen-binding affinities (nmol/L–pmol/L range) and owing to their elongated complementarity-determining region 3 (CDR3) loops, can target hidden or conformational epitopes often inaccessible to conventional antibodies [21,27].
(2) Small size and enhanced tissue penetration: Their small size (~12–15 kDa) facilitates superior tissue penetration, especially in solid tumors, and allows for rapid renal clearance, enhancing the target-to-background ratio and improving diagnostic sensitivity and specificity [19].
(3) Exceptional stability and solubility: Structural features in their framework regions (FR), such as hydrophilic residue substitutions, confer high solubility, resistance to aggregation, and stability under extreme thermal, pH, and enzymatic conditions, enabling robust performance in complex biological environments and facilitating storage and transport (Fig. S2 in Supporting information) [21,26,28].
(4) Low immunogenicity: VHH domains share high sequence homology (~80%) with human VH3 family genes, resulting in low immunogenicity and reduced anti-drug antibody (ADA) responses, which supports their therapeutic use in humans [29].
(5) Cost-effective production and engineering flexibility: Nanobodies are amenable to high-yield microbial expression systems (e.g., Escherichia coli (E. coli), yeast), and their simple architecture enables versatile engineering into multivalent or albumin-fused constructs to enhance pharmacokinetics and function [30].
(6) Suitability for nuclear medicine imaging: Their small size, high stability, rapid clearance, and strong target affinity make nanobodies particularly suitable for radiolabeling in nuclear imaging, outperforming conventional antibodies in signal-to-noise ratio and imaging resolution [31].
Radiotracers based on monoclonal antibodies, small molecules, and peptides each play important roles in molecular imaging but face inherent limitations. Monoclonal antibodies offer high specificity and affinity for tumor antigens but suffer from large size and prolonged circulation, leading to slow tumor penetration and delayed imaging times [14,32,33]. Small molecules provide rapid tumor uptake and deep tissue penetration, yet often lack specificity and are rapidly cleared renally, causing background interference [15,34]. Peptide-based tracers balance these traits with moderate size and receptor specificity [35], enabling faster clearance than mAbs but facing challenges such as lower binding affinity and enzymatic degradation that affect imaging accuracy and signal retention [36]. To systematically evaluate the advantages and limitations of various radiotracer classes, their key properties are summarized in Table S1 (Supporting information).
PET employs radionuclides such as 18F (T1/2 = 110 min), 68Ga (T1/2 = 68 min), and 89Zr (T1/2 = 78.4 h), offering high sensitivity and spatial resolution for molecular imaging [37]. 18F enables efficient, scalable radiolabeling via covalent strategies (e.g., click chemistry) [38], while 68Ga is favored for rapid imaging using chelators like 1,4,7,10-tetraazacyclododecane-1,4,7,10-tetraacetic acid (DOTA), 1,4,7-triazacyclononane-1,4,7-triacetic acid (NOTA), and 1,4,7-triazacyclononane,1-glutaric acid-4,7-acetic acid (NODAGA) [39]. In contrast, the long half-life of 89Zr suits full-length antibodies but is suboptimal for nanobody tracers due to prolonged background retention [40]. SPECT, using γ-emitting isotopes such as 99mTc (T1/2 = 6 h) and 111In (T1/2 = 2.8 d), remains cost-effective and widely accessible. 99mTc is well-suited to nanobody labeling via HYNIC or MAG3, whereas 111In better matches the pharmacokinetics of conventional antibodies than nanobodies [41]. The commonly used radionuclides are listed in Table S2 (Supporting information).
Radiolabeling of nanobodies can be broadly categorized into direct labeling and indirect labeling, each with distinct advantages and limitations.
Direct radiolabeling involves the covalent attachment of radionuclides to nanobodies via reactive functional groups or chemically modified sites on the nanobody surface [42]. For example, the 5F7 nanobody was directly radioiodinated using the Iodogen method [43]. This approach is characterized by high labeling efficiency, simplified synthesis, and reduced processing time, as it eliminates the need for bifunctional chelators. However, labeling conditions such as high temperatures or harsh chemical environments may negatively impact the biological activity of nanobodies [44].
Indirect labeling employs bifunctional chelators (e.g., DOTA, NOTA, NODAGA) to stably coordinate radionuclides in vivo [45]. Though effective, it involves complex synthesis and may alter nanobody properties while increasing cost [46].
(1) Lysine (Lys)- and glycine (Gly)-based labeling: Lys and random Gly based labeling is the most commonly used method for antibody modification in clinical practice. However, its non-specific nature allows multiple Lys residues to react, potentially affecting the CDRs, weakening antigen binding, and reducing imaging or therapeutic efficacy [47]. To overcome these limitations, site-specific conjugation introduces a unique cysteine into a non-functional nanobody region, enabling selective maleimide coupling [48]. This strategy offers a robust approach for site-specific radiolabeling of nanobodies.
(2) One-pot Al-18F labeling: Traditional 18F labeling often requires harsh conditions unsuitable for sensitive biomolecules like nanobodies. The one-pot Al-18F method forms a stable Al-18F complex with a chelator conjugated to the biomolecule, offering mild conditions, simplicity, and short reaction time. This efficient and versatile strategy has attracted growing interest in PET probe development [49].
(3) Click chemistry-mediated labeling: Click chemistry, known for rapid reactions and high yields, is widely used in radiolabeled probe development. The copper-catalyzed azide-alkyne reaction (CuAAC) is common but limited by copper’s incompatibility with biological systems. To address this, strain-promoted azide-alkyne cycloaddition (SPAAC) was developed [50]. Additionally, the inverse electron-demand Diels–Alder (IEDDA) reaction between tetrazine and trans-cyclooctene offers exceptionally fast kinetics, promoting its broad use in radiopharmaceutical chemistry [51].
(4) Enzyme-mediated labeling: Sortase A (SrtA) recognizes an LPXTG motif and catalyzes ligation to N-terminal oligoglycine-bearing molecules (e.g., GGGGK), enabling site-specific 99mTc labeling [52]. Similarly, microbial transglutaminase (mTGase) targets a C-terminal glutamine, forming stable amide bonds with primary amines for efficient, mild labeling [53].
(5) Pretargeting strategies: Pre-targeting enhances nanobody imaging specificity and contrast by separating targeting and radiolabeling, reducing non-specific radiation and off-target accumulation [54]. It suits short-lived radionuclides and rapid nanobody kinetics, enabling flexible multi-modal and multi-target imaging for broader diagnostic and therapeutic use [55].
Here, we categorize the major applications of nanobody-based radiotracers into three domains: Tumor imaging, neuroimaging, and imaging of other diseases (Tables S3 and S4 in Supporting information). We further discuss the advantages and limitations of representative tracers from both research and translational perspectives.
(1) HER2-targeted nanobody radiotracers
HER2 is a receptor tyrosine kinase belonging to the EGFR family, and its overexpression is associated with various malignancies, including breast cancer, gastric cancer, and lung cancer [56-58]. While mAbs such as trastuzumab have been successfully utilized in HER2-positive breast cancer therapy [57,58], challenges such as HER2 heterogeneity and low HER2 expression in certain tumors necessitate the development of highly sensitive, non-invasive molecular imaging approaches to optimize HER2-targeted treatment strategies.
[68Ga]Ga-NOTA-2Rs15d, the first HER2-specific nanobody PET tracer to enter clinical trials, demonstrated high tumor uptake and rapid blood clearance in HER2-positive breast cancer patients during a Phase Ⅰ clinical trial (NCT03331601). The study was further expanded in Phase Ⅱ trials (NCT03331601, NCT03924466) to evaluate its imaging efficacy in brain metastases and other HER2-expressing malignancies [59]. However, significant renal uptake of this tracer may limit its sensitivity for abdominal imaging. In contrast, [99mTc]Tc-NM-02, a SPECT-based imaging agent, exhibited lower off-target renal accumulation in a Phase Ⅰ clinical study (NCT04040686) and demonstrated improved sensitivity in detecting metastatic breast cancer, particularly in lesions with low HER2 expression or high heterogeneity [60].
(2) CEA-targeted nanobody radiotracers
Carcinoembryonic antigen (CEA, CEACAM5) is an important tumor biomarker for malignancies such as colorectal cancer (CRC) and gastric cancer [61,62]. [68Ga]Ga-HNI01, a CEA-targeted PET tracer, has demonstrated low immunogenicity, high tumor contrast, and rapid clearance, enabling high-quality imaging within 30 min. However, its elevated renal and normal colon tissue uptake may compromise the sensitivity of abdominal lesion detection [63]. Another promising CEA-targeted nanobody, Nb41, has been explored for both PET imaging and near-infrared fluorescence (NIRF) intraoperative navigation imaging. Preclinical studies indicate efficient tumor accumulation and prolonged retention, suggesting its potential for precision-guided CRC resection [64].
(3) Trop2-targeted nanobody radiotracers
Trophoblast cell surface antigen 2 (Trop2) is a broadly expressed tumor marker implicated in multiple epithelial cancers. A nanobody-based PET tracer, [68Ga]Ga-NOTA-T4, was recently developed to enable noninvasive imaging of Trop2 expression heterogeneity in both preclinical tumor models and ten patients with solid tumors (NCT06203574) [65]. To optimize pharmacokinetics, a milder [18F]AlF-RESCA labeling strategy was used to develop [18F]AlF-RESCA-T4 and its His-tag–free variant RT4, both exhibiting improved in vivo performance and clinical translation potential [66].
(4) CD70-targeted nanobody radiotracers
CD70 is highly expressed in over 80% of clear cell renal cell carcinomas (ccRCC), but shows minimal distribution in normal tissue [67]. Based on this, Wei et al. developed[18F]RCCB6, a CD70-targeted nanobody-based PET tracer, which demonstrated effective detection of tumor burden and metastases in ccRCC patients (NCT06148220) [68]. To address elevated renal signals, removal of the His-tag significantly reduced non-specific renal uptake (SUVmax = 56) while maintaining high tumor accumulation (SUVmax = 129) [69-71]. This highlights the value of molecular engineering in improving imaging contrast for renal malignancies.
(1) Nanobody-based radiotracers targeting stromal cells
Fibroblast activation protein (FAP) serves as a specific marker of cancer-associated fibroblasts (CAFs) and is overexpressed in the stroma of more than 90% of epithelial malignancies [72-74]. The Xu research team engineered the anti-FAP nanobody AMS002–1 [75]. The radiolabeled derivative, [89Zr]Zr-AMS002–1-Fc, demonstrated high tumor affinity for FAP-positive tumors. As shown in Fig. S3 (Supporting information), another promising FAP-targeting nanobody, 4AH29, was investigated by the Dekempeneer research team [76] (Fig. S3A). This nanobody exhibits sub-nanomolar affinity for both human and murine FAP (Fig. S3B), while maintaining enzymatic activity (Fig. S3C). Radiolabeled [68Ga]Ga-DOTA-4AH29 and [131I]I-GMIB-4AH29 successfully enabled specific imaging of FAP-positive tumors in murine models (Figs. S3D and E). However, both [131I]I-GMIB-4AH29 and [225Ac]Ac-DOTA-4AH29 exhibited notable nephrotoxicity during treatment, highlighting the need for future studies to optimize dosing strategies and mitigate renal toxicity to improve clinical applicability.
(2) Nanobody-based radiotracers targeting extracellular matrix (ECM) proteins
In the tumor microenvironment (TME), ECM remodeling promotes cancer growth, invasion, and immune evasion [77,78]. NJB2 is a promising candidate for diagnostic imaging. The anti-ECM nanobody NJB2 enables PET/CT imaging of primary and metastatic lesions in models of breast cancer, melanoma, and pancreatic ductal adenocarcinoma (PDAC) within 2 h, outperforming conventional [18F]F-FDG PET/CT. Additionally, NJB2 facilitates lesion detection in bleomycin-induced pulmonary fibrosis models, highlighting its potential as a broad-spectrum imaging agent.
Angiogenesis is essential for tumor growth and metastasis, with vascular endothelial growth factor2 (VEGFR2) and neuropilin-1 (NRP-1) as key regulators highly expressed in tumor vasculature. VEGFR2’s limited presence in normal vessels makes it a prime target for anti-angiogenic therapy [79,80]. The Karami research team screened a camel-derived immune nanobody library and successfully identified nanobody candidates with high specificity and nanomolar-level affinity for both VEGFR2 and NRP-1 [81]. These nanobodies exhibited promising efficacy in both in vitro and in vivo models, demonstrating their potential as novel tools for tumor vascular imaging and targeted therapy. Future studies are expected to explore the integration of these nanobody-based probes with multimodal imaging technologies, such as PET and fluorescence imaging, to enable precise tumor visualization and facilitate theranostic applications.
(1) CD8-targeted nanobody radiotracers
CD8 is a key immune marker expressed on cytotoxic T cells, and its infiltration level within tumors serves as an important indicator for evaluating immunotherapy efficacy [82]. [68Ga]Ga-NOTA-SNA006a, synthesized through condensation coupling (Fig. S4A in Supporting information), demonstrated high specificity and affinity for CD8+ T cells both in vitro and in vivo (Figs. S4B and C in Supporting information) [83]. Researchers engineered a variant, [68Ga]Ga-NOTA-SNA006a, by eliminating the His6 tag from [68Ga]Ga-NOTA-SNA006a. The improved probe successfully quantified CD8+ T-cell distribution in Phase Ⅰ clinical trials (NCT05126927), providing valuable insights for assessing tumor immunotherapy responses and developing personalized treatment strategies [84].
(2) CD38-targeted nanobody radiotracers
CD38 is a transmembrane glycoprotein widely expressed in immune and epithelial cells and is overexpressed in multiple malignancies, including multiple myeloma (MM). However, current imaging techniques exhibit limited sensitivity in detecting minimal residual disease (MRD) [85]. In preclinical studies, the nanobody 2F8 demonstrated strong targeting and imaging capability for CD38-positive tumor cells following radiolabeling, along with significant therapeutic efficacy in a CD38-positive MM xenograft model [86]. Additionally, [68Ga]Ga-NOTA-Nb1053, an immunoPET imaging probe, exhibited robust imaging performance in both subcutaneous and orthotopic MM lesions [87,88]. Despite promising preclinical and early clinical findings, CD38-targeted nanobody-based PET/SPECT imaging remains in the early stages of clinical validation, warranting further trials to establish safety and efficacy.
(3) PD-L1-targeted nanobody radiotracers
PD-L1 is a widely studied immune checkpoint molecule that is highly expressed in various tumors and contributes to immune evasion within the TME [89]. Molecular imaging probes targeting the PD-1/PD-L1 axis have made significant strides in both clinical and preclinical research [90]. These probes not only enable noninvasive assessment of PD-1/PD-L1 expression within tumors but also reveal spatial heterogeneity in the TME, offering potential for precise patient stratification and response prediction in immunotherapy. For example, the SPECT tracer [99mTc]Tc-NM-01 has enabled accurate visualization of PD-L1 expression in non-small cell lung cancer (NSCLC) within 2 h post-injection (NCT02978196) [91], improving the identification of responders. Ongoing Phase Ⅰ (NCT04436406) and Phase Ⅱ (NCT04992715) trials are further evaluating its predictive value for PD-1 blockade therapy [92,93].
Meanwhile, the PET tracer [68Ga]Ga-APN09 showed strong correlation with PD-L1 immunohistochemistry (NCT05156515) [94]. Building on this progress, researchers have explored strategies to enhance imaging quality and clinical utility by improving in vivo probe performance. For instance, based on the nanobody RW102, incorporation of an albumin-binding domain (ABD035) extended blood circulation time. Compared to unmodified [68Ga]Ga-NOTA-RW102, the modified tracers [64Cu]Cu-NOTA-ABDRW102 and [89Zr]Zr-DFO-ABDRW102 exhibited higher tumor uptake and improved in vivo stability (NCT06165874), supporting increased imaging sensitivity and delayed imaging capabilities for PD-L1 visualization [95].
(1) Tau-targeted nanobody radiotracers
β-Amyloid peptide (Aβ) and Tau protein are two hallmark pathological features of Alzheimer’s disease (AD) [96], characterized by extracellular plaque deposition and intracellular neurofibrillary tangles (NFTs), respectively [97]. Among these, Tau protein deposition exhibits a stronger correlation with cognitive decline and neurodegeneration [98]. A nanobody named 2C5 (isoelectric point: 7.18) exhibits high affinity and specificity for tau oligomers. Radiolabeling via a tricarbonyl approach yielded [99mTc]Tc-2C5 with high radiochemical purity, good stability. However, brain uptake in healthy mice remained low at 5, 10 and 15 min post-injection, potentially due to its relatively low pI, negative logP value, and the use of non-pathological models. Prior studies show blood–brain barrier (BBB) penetration requires higher isoelectric points [14,99], but research on this remains limited. Future work should focus on modifying nanobody properties to improve brain uptake and tau imaging.
(2) Glial fibrillary acidic protein (GFAP)-targeted nanobody radiotracers
GFAP is a key marker of reactive astrocytes and neuroinflammation [100,101]. To enable targeted imaging, Li et al. developed a nanobody E9 with high specificity for GFAP, capable of crossing the BBB and labeling astrocytes in the brain [99]. To enhance brain uptake, Morito et al. fused E9 with a brain shuttle peptide ApoE (159–167)2 using flexible (EGA) and rigid (EEA) linkers. Among the resulting radiotracers, [18F]F-EEA showed higher GFAP affinity and lower nonspecific binding, though PET failed to reveal clear regional differences, possibly due to low dose or background signal interference [101].
The BBB limits molecular access to the central nervous system (CNS), complicating neuroimaging and therapy [102]. To overcome this, nanobody-based shuttles targeting receptors like TfR have been developed [103,104]. Sehlin et al. created a TfR1-binding nanobody TXB2 and fused it to the anti-Aβ antibody bapineuzumab (Bapi), forming Bapi-TXB2. Radiolabeled [125I]I-Bapi-TXB2 showed strong TfR1 affinity and enabled enhanced BBB penetration, achieving threefold higher brain uptake than [125I]I-Bapi in wild-type mice. In ArcSwe transgenic mice, it exhibited more uniform brain distribution, highlighting its potential to improve CNS delivery while reducing systemic exposure.
Vascular cell adhesion molecule-1 (VCAM-1, CD106) is a 90 kDa glycoprotein expressed on endothelial cells [105], playing a pivotal role in diseases such as atherosclerosis, chronic hepatitis and cancer [106-111]. Broisat et al. developed a high-affinity nanobody, cAbVCAM1–5, with cross-reactivity to human and murine VCAM-1. [99mTc]Tc-cAbVCAM1–5 enabled SPECT imaging in ApoE-/- mice, demonstrating strong lesion uptake that correlated with disease severity, indicating its sensitivity as a tool for monitoring atherosclerotic lesions. In non-alcoholic fatty liver disease (NAFLD) models, [99mTc]Tc-cAbVCAM1–5 sensitively detected hepatic inflammation and monitored its progression and resolution [111].
Dipeptidyl peptidase 6 (DPP6) has been identified as a specific marker for pancreatic β-cells and α-cells [112,113]. Balhuizen et al. developed the nanobody 4hD29, which specifically binds to DPP6 [113]. In immunodeficient mice, SPECT/CT imaging using [99mTc]Tc-4hD29 demonstrated highly specific binding to DPP6-expressing human pancreatic islets and Kelly neuroblastoma cells, with minimal background signal [114]. However, given that DPP6 is expressed in both β-cells and α-cells, the use of this tracer may limit the precise quantification of β-cell mass [115].
Complement receptor Ig superfamily (CRIg) is a biomarker of synovial resident macrophages, and its expression is significantly upregulated in the synovium of rheumatoid arthritis (RA) patients [116]. Zheng et al. developed the nanobody NbV4m119, which specifically targets CRIg [117]. In collagen-induced arthritis (CIA) mouse models, [99mTc]Tc-NbV4m119 uptake was found to correlate with arthritis severity scores, with the tracer successfully detecting early inflammatory signals in asymptomatic mice. These findings suggest that [99mTc]Tc-NbV4m119 may serve as an effective tool for the early prediction, diagnosis, and therapeutic monitoring of RA.
While nanobody-based radiotracers offer unique advantages in nuclear medicine imaging, their clinical translation faces several challenges.
Due to their small molecular size, nanobodies undergo rapid glomerular filtration and subsequent tubular reabsorption, leading to high renal accumulation. Particularly in urogenital tumors such as renal, bladder, and prostate cancers, high background signals in the kidneys may obscure lesions or interfere with delineation of tumor margins, significantly compromising diagnostic accuracy [118]. Therefore, mitigating renal uptake remains a critical challenge for the clinical translation of nanobody radiotracers.
Several strategies have been explored to reduce renal retention. Co-administration of lysine or plasma expanders such as GelofusineⓇ has been shown to reduce renal retention of radiotracers by competitively inhibiting reabsorption through endocytic receptors like megalin and cubulin. GelofusineⓇ reduced the radiation dose of [99mTc]Tc-NM-02 to the kidneys by nearly 50% (0.06 ± 0.007 vs. 0.129 mSv/MBq) in breast cancer patients [119-121].
Amino acid tags are widely used for the expression and purification of antibodies and nanobodies. However, the incorporation of charged amino acid tags can significantly alter the polarity of nanobodies, thereby influencing their biodistribution. Removal of the His-tag has been proposed to reduce tubular reabsorption by minimizing interactions with anionic renal receptors. This strategy effectively decreases non-specific renal retention (cortical SUVmax = 56) without compromising tumor uptake (SUVmax = 129) [71], offering a practical approach to enhance the diagnostic accuracy of primary renal cancers.
Another promising strategy to reduce renal retention involves site-specific radiolabeling using cleavable linkers that are sensitive to renal brush border enzymes (RBBEs). Zhou et al. utilized click chemistry to incorporate an RBBE-cleavable Gly–Lys linker into nanobodies, which promotes the formation of radiometabolites with membrane permeability or low reabsorption, enabling rapid urinary excretion and reducing renal radioactivity by 5-6-fold [122].
Furthermore, PEGylation and albumin-binding modifications have been shown to effectively reduce renal retention of nanobodies by enhancing hydrophilicity and modulating molecular size. Short-chain PEG reduces renal radioactivity by 4-6-fold, while longer chains improve clearance but significantly impair target binding due to steric hindrance. Balancing high tumor targeting with low renal toxicity remains critical. In Zhang et al.’s study, incorporation of ABD035 decreased renal accumulation by 2.2-fold, representing a promising method to mitigate renal toxicity [123,124].
While rapid systemic clearance of nanobodies enhances imaging contrast, it may hinder applications such as radionuclide therapy. Optimizing the pharmacokinetic profile of nanobody tracers is crucial for enhancing their clinical performance.
As previously described, PEGylation forms a steric shield that protects nanobodies from proteolytic degradation, and simultaneously increases their hydrodynamic size, thereby reducing rapid renal clearance [124]. In comparison, fusion with ABD or IgG-binding domain (IgBD) offers a more advantageous strategy [64,125,126]. After binding to albumin, Nb-ABD undergoes neonatal Fc receptor (FcRn)-mediated recycling, extending blood circulation and reducing renal uptake. For example, Zhang et al. reported that conjugation of ABD035 to the nanobody increased the blood circulation of [68Ga]Ga-NOTA-ABDC2 by 13.9-fold [64,123]. Similarly, a novel IgG-binding nanobody, [99mTc]Tc-MIRC213–709, exhibited distribution and elimination half-lives (T1/2α and T1/2β) that were 6.74- and 19.04-fold longer, respectively, compared to the control [127].
PASylation, a strategy involving the attachment of proline-, alanine-, and serine‑rich sequences to nanobody surfaces, increases hydrophilicity and molecular size, reducing renal clearance and extending systemic half-life [128]. Yang et al. provided compelling evidence that the half-life of PASylated nanobodies is 3.8 times that of unmodified nanobodies (0.96 h vs. 0.25 h) [129]. Furthermore, adjusting the injected dose and optimizing the imaging time window can enhance image quality. For instance, modifying the timing of PET/SPECT imaging based on tracer kinetics may allow for improved signal-to-background ratios, ensuring optimal diagnostic performance across various clinical scenarios [45].
Although VHHs share structural similarity with human VH3 domains and generally exhibit low immunogenicity, repeated administration in therapeutic settings can still trigger ADA responses, potentially compromising bioactivity and efficacy. Minimizing immunogenicity is therefore critical for the long-term clinical use of nanobody-based radiotracers. Clinical data from over 35 trials involving more than 1000 subjects report ADA rates ranging from 0% to 30%, with neutralizing ADAs occurring in fewer than 3% of cases, typically transient and treatment-induced [130].
Humanization remains the primary strategy to reduce nanobody immunogenicity. This includes CDR grafting, transferring camelid CDRs onto human antibody frameworks to retain specificity while reducing immune recognition, and framework engineering to further align non-essential residues with human sequences. However, the impact of humanization on immunogenicity is not always predictable. For example, the humanized nanobody Vobarilizumab (ALX-0061) induced no ADAs in a 24-week Phase Ⅰ/Ⅱ trial in RA patients [131], but treatment-emergent ADAs appeared in 31% of patients in Phase Ⅱb [132,133]. Balancing humanization with structural stability and antigen affinity remains a key challenge in nanobody design. Alternative approaches, such as fully human nanobody libraries generated via phage display or AI-guided design, may help bypass immune responses associated with non-human sequences. PEGylation is another option to shield immunogenic epitopes, though careful optimization is needed to preserve functional binding [126].
Effective imaging of central nervous system (CNS) diseases is hindered by the BBB, which restricts the penetration of most antibodies and radiotracers into brain tissue. Although nanobodies possess some degree of BBB permeability due to their small size, additional modifications are needed to enhance CNS targeting efficiency.
One promising strategy involves transferrin receptor (TfR)-mediated transport, wherein nanobodies fused with anti-TfR nanobodies utilize receptor-mediated transcytosis to achieve efficient brain uptake [134]. Similarly, brain shuttle peptides such as Angiopep-2 and ApoE-derived sequences have been employed to enhance nanobody delivery across the BBB [101]. Studies suggest that increasing the pI of nanobodies (>8.5) may also facilitate BBB penetration [99]. Furthermore, nanocarrier-based delivery systems, including liposomes, polymer nanoparticles, and exosomes, have been investigated as potential vehicles for enhancing CNS-specific targeting [103].
The stability of radiolabeling is a critical determinant of tracer specificity, imaging quality, and safety. Unstable labeling can result in radionuclide dissociation, leading to unintended accumulation in non-target tissues, such as bone deposition of free 89Zr. Such off-target effects not only degrade imaging contrast but may also increase radiation toxicity.
Chelator selection plays a pivotal role in maintaining radiolabel stability [45]. While DOTA is widely used for therapeutic radionuclides (177Lu, 225Ac), its affinity for 68Ga is suboptimal. NOTA and NODAGA provide superior 68Ga binding stability, making them preferable choices for PET imaging. For 89Zr-based tracers, traditional deferoxamine (DFO) chelation is associated with limited affinity, prompting the development of modified DFO derivatives (e.g., DFO*) to improve stability and reduce bone uptake [135].
Site-specific labeling techniques, such as C-terminal cysteine conjugation, help minimize batch-to-batch heterogeneity and improve in vivo distribution predictability [136]. In certain cases, co-administration of blocking agents may further decrease non-specific tissue uptake, thereby improving imaging contrast [137].
Despite the promising preclinical performance of nanobody-based radiotracers, their clinical translation remains constrained by several challenges. Chief among these is the limited availability of large-scale clinical validation. To date, only a few nanobody tracers have progressed to clinical trials, such as [68Ga]Ga-NOTA-anti-HER2 nanobody, which has demonstrated high imaging contrast in patients with breast and gastric cancers. However, comparative studies against existing PET tracers (e.g., [68Ga]Ga-PSMA-11 [138]) are necessary to establish whether nanobodies confer significant advantages in terms of target-to-background ratio, imaging kinetics, and diagnostic accuracy.
The production of nanobody radiotracers also presents challenges. The manufacturing process involves recombinant protein expression, purification, radiolabeling, and stringent quality control under good manufacturing practice (GMP) conditions. Expression systems such as E. coli, yeast, and mammalian cells each exhibit distinct trade-offs regarding yield, purification complexity, and cost-effectiveness. Optimization of high-yield, cost-efficient production methods remains a priority.
Furthermore, regulatory approval pathways for nanobody-based radiotracers are not yet fully established. The unique structural properties of nanobodies may necessitate additional safety evaluations beyond those required for conventional monoclonal antibodies or small-molecule tracers. Future efforts should focus on conducting multicenter clinical trials, refining GMP production pipelines, and integrating nanobody imaging with emerging precision medicine strategies such as liquid biopsy to facilitate personalized diagnostics and therapeutics [139].
The future of nanobody-based radiopharmaceuticals in nuclear medicine is poised for significant advancements, driven by innovations in AI, therapeutic applications, and personalized precision medicine.
The integration of AI and machine learning into nanobody research is expected to shift the paradigm from an empirical, trial-and-error approach to a data-driven framework. Currently, nanobody development relies heavily on experimental screening, which is time-consuming and labor-intensive. In contrast, AI-powered deep learning models, combined with protein structure prediction tools such as AlphaFold, will enable precise in silico prediction of nanobody-target interactions, stability, pharmacokinetics, and in vivo biodistribution [140,141]. Such advancements will significantly accelerate the discovery process and facilitate the rational design of nanobody candidates with optimized binding affinity and reduced immunogenicity.
Additionally, AI will play a pivotal role in refining radiolabeling strategies, enhancing nuclide stability, and minimizing off-target effects. By leveraging computational modeling and high-throughput screening, AI-assisted approaches can optimize chelator selection, linker chemistry, and conjugation strategies to improve the pharmacokinetic profile of radiolabeled nanobodies. This technological breakthrough is expected to yield imaging agents with higher specificity and improved signal-to-noise ratios, particularly for challenging-to-image pathologies such as solid tumors and neurodegenerative disorders. Consequently, AI-driven advancements will enhance the early detection and diagnostic accuracy of various diseases, further advancing precision nuclear medicine.
Beyond their diagnostic utility, nanobodies hold immense potential for targeted radionuclide therapy (theranostics) [142]. With the development of therapeutic α- or β-emitting radionuclides such as 177Lu and 225Ac, the clinical translation of theranostic nanobody-based radiopharmaceuticals is expected to accelerate in the near future. Current efforts focus on prolonging blood circulation (e.g., through PEGylation or albumin binding [123]), selecting matched diagnostic-therapeutic radionuclide pairs such as 68Ga and 177Lu, or radionuclides with both diagnostic and therapeutic functions like 131I [143], applying pretargeting strategies to lower toxicity, and reducing liver and kidney uptake by metabolic optimization. These advances help combine imaging and treatment in one agent, improving therapeutic precision and safety [144,145]. Moreover, in the context of brain tumors, nanobody-based radiotherapeutics may offer enhanced BBB permeability compared to conventional antibodies, thereby expanding the potential applications of targeted radionuclide therapy in neuro-oncology.
The development of bifunctional nanobodies for both diagnosis and therapy will simplify patient management by enabling real-time treatment monitoring. Such agents can reduce procedural steps, improving efficiency and compliance. Advances in radionuclide production, nanobody engineering, and delivery systems are expected to accelerate their clinical translation in the coming years.
Precision medicine relies on individualized treatment strategies tailored to the unique molecular and pathological characteristics of each patient. In this context, nanobody-based immunoPET imaging offers high precision in visualizing in vivo target distribution and expression dynamics, and holds clear translational potential. For example, the radiolabeled PD-L1 nanobody [68Ga]Ga-NOTA-RW102 enables noninvasive assessment of the PD-1/PD-L1 axis in cancer patients, facilitating the identification of potential responders and supporting decision-making for immunotherapy. Moreover, with an imaging window spanning from 30 min to 144 h post-injection, this tracer is well-suited for continuous monitoring of treatment response and the emergence of immune-related adverse events [95].
Similarly, the Trop2-specific tracer [68Ga]Ga-NOTA-T4 demonstrates clear visualization of heterogeneous Trop2 expression in solid tumors, aiding in the optimization of therapeutic strategies and adjustment of treatment regimens [65,66]. In addition, integrating molecular imaging with AI-driven predictive models offers the potential for individualized radiation dose estimation, ensuring effective therapy while minimizing radiation exposure to healthy tissues [146]. Looking forward, the development of nanobody tracers capable of capturing immune dynamics in real time will be a key direction for future research and clinical innovation.
Over the next 5–10 years, the synergistic impact of AI-driven nanobody optimization, therapeutic radiolabeled nanobodies, and precision medicine-guided imaging will propel nuclear medicine to new frontiers. These innovations will contribute to more accurate disease diagnosis, more effective radionuclide therapy regimens, and safer, patient-specific treatment strategies. Additionally, the expanding role of nanobody-based radiopharmaceuticals in oncology, neurodegenerative disorders, and immune-related diseases underscores their potential to revolutionize the field of molecular imaging and targeted therapy.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Ying Yao: Writing – original draft, Conceptualization. Juan Tian: Writing – original draft, Conceptualization. Ran Zhang: Writing – original draft. Ping Liu: Writing – original draft. Xiang Gao: Writing – review & editing. Wenhu Zhou: Writing – review & editing, Conceptualization. Longlong Luo: Writing – review & editing.
This work was supported by the National Natural Science Foundation of China (No. 82204262), and Hunan Province College Students Research Learning and Innovative Experiment Project (No. S202410542221).
Supplementary material associated with this article can be found, in the online version, at doi:
Y. Muhammad, M. Tahir, M. Hayat, K.T. Chong, Sci. Rep. 10 (2020) 19747. doi: 10.1038/s41598-020-76635-9
S.C. Vaz, F. Oliveira, K. Herrmann, P. Veit-Haibach, Br. J. Radiol. 93 (2020) 20200095. doi: 10.1259/bjr.20200095
J.J. Zhang, L.J. Lou, R. Lv, et al., Chin. Chem. Lett. 35 (2024) 109342. doi: 10.1016/j.cclet.2023.109342
X.Q. Chen, W.C. Niu, Z.Y. Du, et al., Chin. Chem. Lett. 33 (2022) 3349–3360. doi: 10.1016/j.cclet.2022.02.070
W.A. Weber, J. Clin. Oncol. 24 (2006) 3282–3292. doi: 10.1200/JCO.2006.06.6068
K. Vermeulen, M. Vandamme, G. Bormans, F. Cleeren, Semin. Nucl. Med. 49 (2019) 339–356. doi: 10.1053/j.semnuclmed.2019.07.001
R. Boellaard, M.J. O’Doherty, W.A. Weber, et al., Eur. J. Nucl. Med. Mol. Imaging 37 (2010) 181–200. doi: 10.1007/s00259-009-1297-4
R.L. Wahl, B.A. Siegel, R.E. Coleman, C.G. Gatsonis, J. Clin. Oncol. 22 (2004) 277–285. doi: 10.1200/JCO.2004.04.148
U. Veronesi, C. De Cicco, V.E. Galimberti, et al., Ann. Oncol. 18 (2007) 473–478. doi: 10.1093/annonc/mdl425
K.I. Pritchard, J.A. Julian, C.M. Holloway, et al., J. Clin. Oncol. 30 (2012) 1274–1279. doi: 10.1200/JCO.2011.38.1103
D. Groheux, A. Cochet, O. Humbert, et al., J. Nucl. Med. 57 (2016) 17s–26s. doi: 10.2967/jnumed.115.157859
P. Vasudevan, R. Gäbel, J. Stenzel, et al., Int. J. Mol. Sci. 21 (2020) 3340. doi: 10.3390/ijms21093340
S.M. Knowles, A.M. Wu, J. Clin. Oncol. 30 (2012) 3884–3892. doi: 10.1200/JCO.2012.42.4887
N.A. Jumapili, M. Zivalj, R.M. Barthelmess, et al., Eur. J. Immunol. 53 (2023) e2250024. doi: 10.1002/eji.202250024
A. Kallinen, M. Kassiou, Nucl. Med. Biol. 114-115 (2022) 115–127. doi: 10.1016/j.nucmedbio.2022.04.001
S. Lee, J. Xie, X.Y. Chen, Biochemistry 49 (2010) 1364–1376. doi: 10.1021/bi901135x
P. Cordell, G. Carrington, A. Curd, et al., J. Cell Sci. 135 (2022) 259168. doi: 10.1242/jcs.259168
J.L. Liu, G.P. Anderson, J.B. Delehanty, et al., Mol. Immunol. 44 (2007) 1775–1783. doi: 10.1016/j.molimm.2006.07.299
I. Van Audenhove, J. Gettemans, EBioMedicine 8 (2016) 40–48. doi: 10.1016/j.ebiom.2016.04.028
Y. Vedvyas, J. Gonzalez-Valdivieso, Y. Alcaina, et al., Cancer Res. 82 (2022) 5976-5976. doi: 10.1158/1538-7445.AM2022-5976
M. Dumoulin, K. Conrath, A. Van Meirhaeghe, et al., Protein Sci. 11 (2002) 500–515. doi: 10.1110/ps.34602
E.Y. Yang, K. Shah, Front. Oncol. 10 (2020) 1182. doi: 10.3389/fonc.2020.01182
L.A. Bocancia-Mateescu, D. Stan, A.C. Mirica, et al., Pharmaceuticals 16 (2023) 863. doi: 10.3390/ph16060863
C. Hamers-Casterman, T. Atarhouch, S. Muyldermans, et al., Nature 363 (1993) 446–448. doi: 10.1038/363446a0
J.P. Salvador, L. Vilaplana, M.P. Marco, Anal. Bioanal. Chem. 411 (2019) 1703–1713. doi: 10.1007/s00216-019-01633-4
B.K. Jin, S. Odongo, M. Radwanska, S. Magez, Int. J. Mol. Sci. 24 (2023) 5994. doi: 10.3390/ijms24065994
T. Chanier, P. Chames, Antibodies 8 (2019) 13. doi: 10.3390/antib8010013
J. Davies, L. Riechmann, FEBS Lett. 339 (1994) 285–290. doi: 10.1016/0014-5793(94)80432-X
S. Muyldermans, Annu. Rev. Biochem. 82 (2013) 775–797. doi: 10.1146/annurev-biochem-063011-092449
W.S. Liu, H.P. Song, Q. Chen, et al., Mol. Immunol. 96 (2018) 37–47. doi: 10.1016/j.molimm.2018.02.012
I. Vaneycken, M. D’Huyvetter, S. Hernot, et al., Curr. Opin. Biotechnol. 22 (2011) 877–881. doi: 10.1016/j.copbio.2011.06.009
R. Manafi-Farid, B. Ataeinia, S. Ranjbar, et al., Front. Med. 9 (2022) 916693. doi: 10.3389/fmed.2022.916693
P. Mohr, J. van Sluis, M.N. Lub-de Hooge, et al., Front. Nucl. Med. 4 (2024) 1360710. doi: 10.3389/fnume.2024.1360710
M.S. Hofman, R.J. Hicks, T. Maurer, M. Eiber, Radiographics 38 (2018) 200–217. doi: 10.1148/rg.2018170108
Y.Q. Yan, H. Wang, Y.L. Zhao, Chin. Chem. Lett. 33 (2022) 3361–3370. doi: 10.1016/j.cclet.2022.02.016
Y.C. Toner, A.A. Ghotbi, S. Naidu, et al., Sci. Rep. 12 (2022) 6185. doi: 10.1038/s41598-022-09590-2
J. Schwenck, D. Sonanini, J.M. Cotton, et al., Nat. Rev. Cancer 23 (2023) 474–490. doi: 10.1038/s41568-023-00576-4
S. Nagachinta, P. Novelli, Y. Joyard, et al., Sci. Rep. 12 (2022) 18655. doi: 10.1038/s41598-022-23552-8
J. Schwenck, H. Rempp, G. Reischl, et al., Eur. J. Nucl. Med. Mol. Imaging 44 (2016) 92–101.
G.A.M.S. van Dongen, W. Beaino, A.D. Windhorst, et al., J. Nucl. Med. 62 (2021) 438–445. doi: 10.2967/jnumed.119.239558
J.H. Jiao, J.J. Zhang, W.H. Wen, W.J. Qin, X.Y. Chen, Theranostics 14 (2024) 2736–2756. doi: 10.7150/thno.95039
X.L. Zhong, J.J. Yan, X. Ding, et al., Bioconjug. Chem. 34 (2023) 457–476. doi: 10.1021/acs.bioconjchem.2c00583
M. Pruszynski, E. Koumarianou, G. Vaidyanathan, et al., Nucl. Med. Biol. 40 (2013) 52–59. doi: 10.1016/j.nucmedbio.2012.08.008
Y.Z. Yang, J. Wang, Y. Zhong, M. Tian, H. Zhang, ACS Appl. Mater. Interfaces 17 (2025) 4316–4336. doi: 10.1021/acsami.4c19059
G. Crișan, N.S. Moldovean-Cioroianu, D.G. Timaru, et al., Int. J. Mol. Sci. 23 (2022) 5023. doi: 10.3390/ijms23095023
W.J. Wei, Z.T. Rosenkrans, J.J. Liu, et al., Chem. Rev. 120 (2020) 3787–3851. doi: 10.1021/acs.chemrev.9b00738
R. Fay, J.P. Holland, J. Nucl. Med. 60 (2019) 587–591. doi: 10.2967/jnumed.118.220806
D.M. Chigoho, Q. Lecocq, R.M. Awad, et al., Pharmaceuticals 14 (2021) 550. doi: 10.3390/ph14060550
S.J. Archibald, L. Allott, EJNMMI Radiopharm. Chem. 6 (2021) 30. doi: 10.1186/s41181-021-00141-0
D. Bauer, M.A. Cornejo, T.T. Hoang, J.S. Lewis, B.M. Zeglis, Bioconjug. Chem. 34 (2023) 1925–1950. doi: 10.1021/acs.bioconjchem.3c00286
C. Canovas, M. Moreau, J.M. Vrigneaud, et al., Bioconjug. Chem. 30 (2019) 888–897. doi: 10.1021/acs.bioconjchem.9b00017
Q. Luo, H. Gao, J. Shi, F. Wang, Biophys. Rep. 7 (2021) 295–303. doi: 10.52601/bpr.2021.210012
Y. Yang, Z. Ren, D. Wang, et al., ACS Nano 19 (2025) 439–450. doi: 10.1021/acsnano.4c09127
A. Forero, P.L. Weiden, J.M. Vose, et al., Blood 104 (2004) 227–236.
Z.X. Chen, M. Chen, K.X. Zhou, J.H. Rao, Angew. Chem. Int. Ed. 59 (2020) 7864–7870. doi: 10.1002/anie.201916352
D.J. Slamon, G.M. Clark, S.G. Wong, et al., Science 235 (1987) 177–182. doi: 10.1126/science.3798106
C.S. Wynn, S.C. Tang, Cancer Metastasis Rev. 41 (2022) 193–209. doi: 10.1007/s10555-022-10021-x
T. Vu, F.X. Claret, Front. Oncol. 2 (2012) 62.
M. Keyaerts, C. Xavier, J. Heemskerk, et al., J. Nucl. Med. 57 (2016) 27–33. doi: 10.2967/jnumed.115.162024
L.Z. Zhao, C.C. Liu, Y. Xing, et al., Mol. Pharm. 18 (2021) 3616–3622. doi: 10.1021/acs.molpharmaceut.1c00569
Z.W. Han, Z.W. Lyv, B. Cui, et al., Invest. New Drugs 38 (2020) 1888–1898. doi: 10.1007/s10637-020-00955-w
N. Beauchemin, A. Arabzadeh, Cancer Metastasis Rev. 32 (2013) 643–671. doi: 10.1007/s10555-013-9444-6
L.Q. Li, X.F. Lin, L. Wang, et al., Eur. J. Nucl. Med. Mol. Imaging 50 (2023) 3735–3749. doi: 10.1007/s00259-023-06313-1
Y.T. Xiao, C.M. Mei, D. Xu, et al., Eur. J. Nucl. Med. Mol. Imaging 50 (2023) 2305–2318. doi: 10.1007/s00259-023-06183-7
W. Huang, Y. Zhang, M. Cao, et al., EMBO Mol. Med. 16 (2024) 1143–1161. doi: 10.1038/s44321-024-00059-5
W. Huang, M. Cao, Y.F. Wu, et al., J. Nucl. Med. 65 (2024) 1904–1910.
W.J. Wei, V. Grünwald, K. Herrmann, Med 6 (2025) 100671. doi: 10.1016/j.medj.2025.100671
X. Zhou, Q.Y. Wu, W. Zhai, et al., J. Nucl. Med. 65 (2024) 1891–1898.
Q.Y. Wu, Y.F. Wu, Y. Zhang, et al., Eur. Urol. 86 (2024) 372–374. doi: 10.1016/j.eururo.2024.06.020
Q.Y. Wu, Y.F. Wu, Y. Zhang, et al., Eur. J. Nucl. Med. Mol. Imaging 51 (2024) 2444–2457. doi: 10.1007/s00259-024-06672-3
S. Wu, Q.Y. Wu, J.J. Liu, J. Zhang, W.J. Wei, Eur. J. Nucl. Med. Mol. Imaging 52 (2025) 1944–1945. doi: 10.1007/s00259-024-07001-4
K. Aertgeerts, I. Levin, L.H. Shi, et al., J. Biol. Chem. 280 (2005) 19441–19444. doi: 10.1074/jbc.C500092200
A.A. Fitzgerald, L.M. Weiner, Cancer Metastasis Rev. 39 (2020) 783–803. doi: 10.1007/s10555-020-09909-3
L. Zhao, F. Kang, Y.Z. Pang, et al., J. Nucl. Med. 65 (2024) 4S–11S. doi: 10.2967/jnumed.123.266983
J.F. Xu, S.H. Li, S.S. Xu, et al., Cancer Biother. Radiopharm. 38 (2023) 726–737. doi: 10.1089/cbr.2021.0389
Y. Dekempeneer, S. Massa, F. Santens, et al., J. Nucl. Med. 64 (2023) 1941–1948. doi: 10.2967/jnumed.123.266381
R.O. Hynes, Science 326 (2009) 1216–1219. doi: 10.1126/science.1176009
N. Jailkhani, J.R. Ingram, M. Rashidian, et al., Proc. Natl. Acad. Sci. U. S. A. 116 (2019) 14181–14190. doi: 10.1073/pnas.1817442116
S.A. Patel, M.B. Nilsson, X.N. Le, et al., Clin. Cancer Res. 29 (2023) 30–39. doi: 10.1158/1078-0432.ccr-22-1366
L.H. Li, X. Jiang, Q. Zhang, et al., J. Exp. Clin. Cancer Res. 35 (2016) 16. doi: 10.1186/s13046-016-0291-5
E. Karami, S. Naderi, R. Roshan, M. Behdani, F. Kazemi-Lomedasht, Cancer Chemother. Pharmacol. 89 (2022) 165–172. doi: 10.1007/s00280-021-04372-5
M. Philip, A. Schietinger, Nat. Rev. Immunol. 22 (2022) 209–223. doi: 10.1038/s41577-021-00574-3
H.T. Zhao, C. Wang, Y.L. Yang, et al., J. Nanobiotechnology 19 (2021) 42. doi: 10.1186/s12951-021-00785-9
Y. Wang, C. Wang, M.Z. Huang, et al., Eur. J. Nucl. Med. Mol. Imaging 49 (2022) 4394–4405. doi: 10.1007/s00259-022-05903-9
J. Puttemans, B. Stijlemans, M. Keyaerts, et al., Mol. Cancer Ther. 21 (2022) 159–169. doi: 10.1158/1535-7163.mct-21-0220
E. Duray, M. Lejeune, F. Baron, et al., J. Hematol. Oncol. 14 (2021) 183. doi: 10.1186/s13045-021-01171-6
C. Wang, Y.M. Chen, Y.N. Hou, et al., Eur. J. Nucl. Med. Mol. Imaging 48 (2021) 2749–2760. doi: 10.1007/s00259-021-05218-1
W.J. Wei, D. Zhang, C. Wang, et al., Mol. Pharm. 19 (2022) 3502–3510. doi: 10.1021/acs.molpharmaceut.1c00733
M.J. Butte, M.E. Keir, T.B. Phamduy, A.H. Sharpe, G.J. Freeman, et al., Immunity 27 (2007) 111–122. doi: 10.1016/j.immuni.2007.05.016
A.M. Paterson, K.E. Brown, M.E. Keir, et al., J. Immunol. 187 (2011) 1097–1105. doi: 10.4049/jimmunol.1003496
Y. Xing, G. Chand, C.C. Liu, et al., J. Nucl. Med. 60 (2019) 1213–1220. doi: 10.2967/jnumed.118.224170
G. Chand, D. Hughes, L. Meszaros, et al., J. Nucl. Med. 65 (2024) 241489.
D. Hughes, G. Chand, L. Meszaros, et al., J. Nucl. Med. 63 (2022) 2594.
X.P. Ma, X. Zhou, B. Hu, et al., Eur. J. Nucl. Med. Mol. Imaging 50 (2023) 3838–3850. doi: 10.1007/s00259-023-06373-3
Y. Zhang, M. Cao, Y.F. Wu, et al., J. Immunother. Cancer 12 (2024) e008794. doi: 10.1136/jitc-2024-008794
Y.Y. Li, T.Q. Liu, M.C. Cui, Chin. Chem. Lett. 33 (2022) 3339–3348. doi: 10.1016/j.cclet.2022.03.024
N. De Leiris, P. Perret, C. Lombardi, et al., J. Transl. Med. 22 (2024) 163. doi: 10.1186/s12967-024-04987-1
N.A. Jackson, M.J. Guerrero-Muñoz, D.L. Castillo-Carranza, Front. Aging Neurosci. 14 (2022) 974414. doi: 10.3389/fnagi.2022.974414
T.F. Li, J.P. Bourgeois, S. Celli, et al., FASEB J. 26 (2012) 3969–3979. doi: 10.1096/fj.11-201384
C. Escartin, E. Galea, A. Lakatos, et al., Nat. Neurosci. 24 (2021) 312–325. doi: 10.1038/s41593-020-00783-4
T. Morito, R. Harada, R. Iwata, et al., PLoS One 18 (2023) e0287047. doi: 10.1371/journal.pone.0287047
W.M. Pardridge, Expert Opin. Drug Deliv. 13 (2016) 963–975. doi: 10.1517/17425247.2016.1171315
G.C. Terstappen, A.H. Meyer, R.D. Bell, W. Zhang, Nat. Rev. Drug Discov. 20 (2021) 362–383. doi: 10.1038/s41573-021-00139-y
D. Sehlin, P. Stocki, T. Gustavsson, et al., FASEB J. 34 (2020) 13272–13283. doi: 10.1096/fj.202000610rr
G.E. Rice, M.P. Bevilacqua, Science 246 (1989) 1303–1306. doi: 10.1126/science.2588007
C. Cerutti, A.J. Ridley, Exp. Cell Res. 358 (2017) 31–38. doi: 10.1016/j.yexcr.2017.06.003
D.H. Kong, Y.K. Kim, M.R. Kim, J.H. Jang, S. Lee, Int. J. Mol. Sci. 19 (2018) 1057. doi: 10.3390/ijms19041057
A. Moreau, E. Varey, I. Anegon, M.C. Cuturi, Cold Spring Harb. Perspect. Med. 3 (2013) a015461. doi: 10.1101/cshperspect.a015461
G.W. Fearnley, A.F. Odell, A.M. Latham, et al., Mol. Biol. Cell 25 (2014) 2509–2521. doi: 10.1091/mbc.e14-05-0962
A. Broisat, S. Hernot, J. Toczek, et al., Circ. Res. 110 (2012) 927–937. doi: 10.1161/CIRCRESAHA.112.265140
M. Nachit, C. Montemagno, R. Clerc, et al., Nat. Commun. 14 (2023) 1062. doi: 10.1038/s41467-023-36776-7
L. Lin, J.G. Murphy, R.M. Karlsson, et al., Front. Cell Neurosci. 12 (2018) 84.
A. Balhuizen, S. Massa, I. Mathijs, et al., Sci. Rep. 7 (2017) 15130. doi: 10.1038/s41598-017-15417-2
S. Demine, R. Garcia Ribeiro, J. Thevenet, et al., Diabetologia 63 (2020) 825–836. doi: 10.1007/s00125-019-05068-5
Z. Li, H.Z. Lei, Z.Q. Ren, et al., Chin. Chem. Lett. 36 (2025) 110804. doi: 10.1016/j.cclet.2024.110804
S.Y. Tao, H. Yu, T. You, et al., ACS Nano 17 (2023) 13917–13937. doi: 10.1021/acsnano.3c03828
F. Zheng, S. Put, L. Bouwens, et al., J. Nucl. Med. 55 (2014) 824–829. doi: 10.2967/jnumed.113.130617
Q.Y. Wu, G. Huang, W.J. Wei, J.J. Liu, Mol. Pharm. 19 (2022) 3457–3470. doi: 10.1021/acs.molpharmaceut.2c00034
L.O. Gainkam, V. Caveliers, N. Devoogdt, et al., Contrast Media Mol. Imaging 6 (2011) 85–92. doi: 10.1002/cmmi.408
B. Altunay, A. Goedicke, O.H. Winz, et al., Eur. J. Nucl. Med. Mol. Imaging 50 (2023) 1005–1013. doi: 10.1007/s00259-022-06066-3
M. D’Huyvetter, C. Vincke, C. Xavier, et al., Theranostics 4 (2014) 708–720. doi: 10.7150/thno.8156
Z.Y. Zhou, N. Devoogdt, M.R. Zalutsky, G. Vaidyanathan, Bioconjug. Chem. 29 (2018) 4090–4103. doi: 10.1021/acs.bioconjchem.8b00699
Y. Zhang, D. Zhang, S.X. An, et al., Research 6 (2023) 0077. doi: 10.34133/research.0077
C.P. Olkowski, F. Basuli, B. Fernandes, et al., Mol. Pharm. 22 (2025) 533–543. doi: 10.1021/acs.molpharmaceut.4c01101
W.Y. Song, W.J. Wei, X.L. Lan, W.B. Cai, Eur. J. Nucl. Med. Mol. Imaging 50 (2023) 2591–2594. doi: 10.1007/s00259-023-06266-5
Y. Vugmeyster, C.A. Entrican, A.P. Joyce, et al., Bioconjug. Chem. 23 (2012) 1452–1462. doi: 10.1021/bc300066a
B. Hu, T.Y. Liu, L.Q. Li, et al., Bioconjug. Chem. 33 (2022) 1328–1339. doi: 10.1021/acs.bioconjchem.2c00209
A. Richter, K. Knorr, M. Schlapschy, et al., Nucl. Med. Mol. Imaging 54 (2020) 114–119. doi: 10.1007/s13139-020-00638-7
Y.C. Yang, L.Y. Jin, Y. Zhang, et al., J. Innov. Opt. Heal. 18 (2024) 2541001.
M.A. Rossotti, K. Belanger, K.A. Henry, J. Tanha, FEBS J. 289 (2022) 4304–4327. doi: 10.1111/febs.15809
J.B. Holz, L. Sargentini-Maier, S. De Bruyn, et al., Ann. Rheum. Dis. 72 (2013) A64.
NCT02287922, 2014.
NCT02437890, 2015.
S.R. Meier, D. Sehlin, S. Syvänen, Nucl. Med. Biol. 114-115 (2022) 121–127.
H.J. Cho, N. Al-Saden, H. Lam, et al., Nucl. Med. Biol. 84-85 (2020) 11–19. doi: 10.1016/j.nucmedbio.2019.12.009
J. Ravasco, H. Faustino, A. Trindade, P.M.P. Gois, Chemistry 25 (2019) 43–59. doi: 10.1002/chem.201803174
M. Müller, L. Lucaroni, N. Favalli, et al., J. Med. Chem. 67 (2024) 8247–8260. doi: 10.1021/acs.jmedchem.4c00332
U. Hennrich, M. Eder, Pharmaceuticals 14 (2021) 713. doi: 10.3390/ph14080713
M.K. Bakht, H. Beltran, Nat. Rev. Urol. 22 (2025) 26–45. doi: 10.1038/s41585-024-00900-z
K.H. Sumida, R. Núñez-Franco, I. Kalvet, et al., J. Am. Chem. Soc. 146 (2024) 2054–2061. doi: 10.1021/jacs.3c10941
A. Ramon, M. Ali, M. Atkinson, et al., Nat. Mach. Intell. 6 (2024) 74–91. doi: 10.1038/s42256-023-00778-3
X.R. Long, S.X. Cheng, X.L. Lan, W.J. Wei, D.W. Jiang, Eur. J. Nucl. Med. Mol. Imaging 52 (2025) 2225–2238. doi: 10.1007/s00259-025-07077-6
M. D’Huyvetter, J. De Vos, C. Xavier, et al., Clin. Cancer Res. 23 (2017) 6616–6628. doi: 10.1158/1078-0432.CCR-17-0310
M. Pruszynski, M. D’Huyvetter, F. Bruchertseifer, A. Morgenstern, T. Lahoutte, Mol. Pharm. 15 (2018) 1457–1466. doi: 10.1021/acs.molpharmaceut.7b00985
E.A.M. Ruigrok, N. van Vliet, S.U. Dalm, et al., Eur. J. Nucl. Med. Mol. Imaging 48 (2021) 1339–1350. doi: 10.1007/s00259-020-05057-6
J.W. Liu, L. Wu, A.Q. Xie, et al., J. Nanobiotechnology 23 (2025) 87. doi: 10.1186/s12951-025-03169-5

 扫一扫看文章
扫一扫看文章

扫一扫关注我们
 DownLoad:
DownLoad:

 下载:
下载:
 下载:
下载: