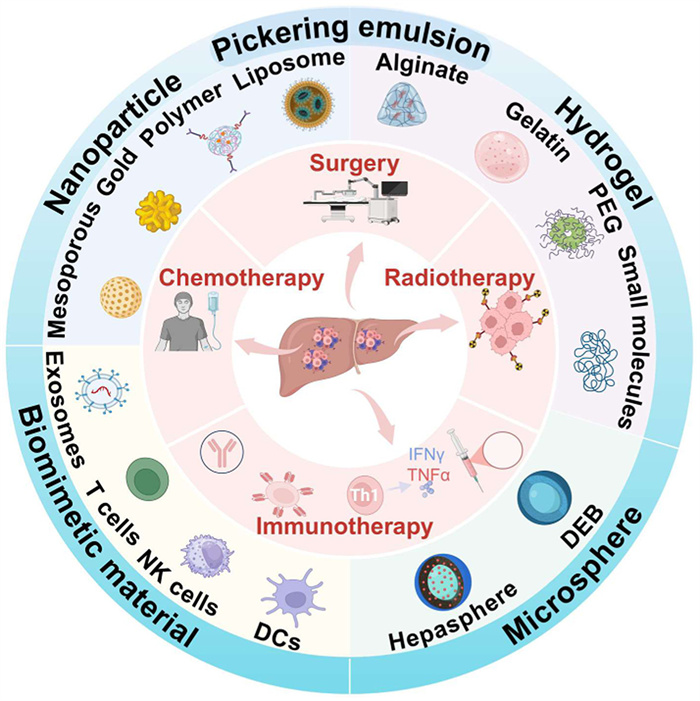
Scheme 1.
Schematic diagram of micro-nanomaterials as drug delivery systems for remodeling the TIME of HCC. Created with BioRender.com.
Micro-nanomaterials-engineered delivery systems for reshaping the tumor immune microenvironment in hepatocellular carcinoma
Mengmeng Miao , Yisheng Peng , Hui Liu , Hu Chen , Xu Cheng , Shangqing Chen , Kaifei Yan , Hongwei Cheng , Gang Liu

Hepatocellular carcinoma (HCC) is among the most prevalent malignancies globally and has significant invasiveness [1]. Although the incidence of HCC has decreased in recent years, its prognosis is still poor, with a five-year survival rate of less than 30% for patients with HCC, and the prevention and treatment of HCC in China is even more severe [2,3]. In-depth mechanism research reveals that the occurrence and development of HCC is not only due to the mutation and malignant proliferation but is also deeply affected by the hepatic immune microenvironment [4]. Consequently, in recent years, immunotherapy and its combination therapy have attracted great attention in the clinical transformation of HCC.
The objective of immunotherapy is to boost the immune system, activate immune cells, and develop tumor-specific immunity against tumors [5]. Immune checkpoint inhibitors (ICIs) represent the most common and effective category of immunotherapeutic agents. Programmed cell death protein 1 and ligand 1 (PD-1/PD-L1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) inhibitors serve as key ICIs. The PD-1 receptor, which is expressed on activated T cells, B cells, and macrophages, could interact with its ligands PD-L1 and PD-L2 to inhibit antigen-specific T-cell activation [6]. The activation of the PD-1/PD-L1 signaling pathway lowers T-cell immune function within the tumor microenvironment (TME), resulting in diminished cytotoxicity and increased tumor progression [7]. PD-1/PD-L1 inhibitors obstruct this interaction, reactivate T cell activity, and enhance their capacity to kill tumor cells [8]. The combination of atezolizumab, a PD-L1 inhibitor, with bevacizumab, a vascular endothelial growth factor (VEGF) inhibitor, has emerged as the principal treatment for advanced HCC. Atezolizumab blocks PD-L1, thereby preventing its interaction with PD-1 and reversing T cell suppression. In contrast, bevacizumab targets VEGF to decrease angiogenesis and tumor progression. This combination has demonstrated encouraging clinical outcomes [9]. In addition to ICIs, additional immunotherapies such as adoptive cell therapy (ACT), tumor vaccines, cytokines, and combination treatments with chemotherapy or targeted therapies have been explored to boost antitumor effectiveness. Despite the promising results, immunotherapy for HCC also faces many challenges. Initially, failure of the immune system to accurately differentiate between healthy and cancerous cells can lead to unintended consequences and reduced treatment efficacy [10]. The heterogeneous characteristics of the HCC immune microenvironment result in varying responses among patients. While certain patients may initially respond favorably to treatment, resistance often develops as tumor cells escape the immune system [11]. Tumor cells employ multiple mechanisms to evade immune detection, presenting a considerable challenge in the treatment of HCC [12]. Moreover, immunotherapy may induce immune-related adverse effects, leading to systemic toxicity that can harm organs, including the liver and gastrointestinal tract. Cytokine release syndrome (CRS) is a common side effect marked by symptoms including fever, hypotension, and respiratory distress [13]. These toxic side effects can significantly impair a patient's quality of life and may be life-threatening in certain instances. To address these issues, further optimization of treatment strategies, exploration of innovative combination therapies, and development of drug delivery system carriers are necessary. These approaches need to focus on a deeper understanding of the immune microenvironment in HCC to enhance the responsiveness to immunotherapy.
The limitations of conventional immunotherapy highlight the urgent need for innovative strategies to improve therapeutic precision and mitigate systemic toxicity. In this context, micro/nanomaterials have emerged as transformative tools to reshape the immunosuppressive TME of HCC. These engineering platforms, which include nanoparticles (NPs), hydrogels, microspheres, biomimetic materials, NPs, or hydrogel-assisted Pickering emulsions, have unparalleled advantages in spatiotemporal control, targeted delivery, and multifunctional integration, making them ideal candidates for addressing the challenges of HCC immunotherapy (Scheme 1). This work begins with a systematic introduction of the immunosuppressive molecular landscape of HCC, emphasizing the key mechanisms that drive immune evasion. Building upon this mechanistic foundation, the review transitions to an in-depth review of micro/nanomaterial-based strategies for remodeling the immunosuppressive microenvironment and enhancing therapeutic efficacy. This review highlights the potential of combinatorial material engineering to accelerate the advancement of next-generation immunotherapies for HCC.
The liver is recognized as an immune tolerance organ, exhibiting immunosuppressive properties, the inhibitory TIME facilitates tumor evasion of the immune response [14]. In HCC, the immunosuppressive state is characterized by the presence of tumor cells, tumor-associated immune cells, and the secreted cytokines and extracellular matrix (ECM) components (Fig. S1 in Supporting information), collectively forming a systematic solid microenvironment [15]. A complex immunosuppressive network is formed through the interaction of various tumor stroma and infiltrating cells, including tumor-associated macrophages (TAMs), cancer-associated fibroblasts (CAFs), regulatory T cells (Tregs), myeloid-derived suppressor cells (MDSCs), and neutrophils linked to tumors (TANs) [16]. In the HCC microenvironment, TAMs are classified as M2-type macrophages, secreting interleukin-10 (IL-10), transforming growth factor β (TGF-β), and VEGF, which facilitate tumor cell growth, suppress immune responses, aid in immune evasion, and promote angiogenesis, thus contributing to the progression of HCC [17,18]. Besides, CAFs are significant components of the tumor stroma, secreting TGF-β and IL-6. These factors play a significant role in developing an immunosuppressive microenvironment, inhibiting effector T-cell functions, reshaping the tumor stroma, and facilitating tumor migration and metastasis [19]. Besides, Tregs diminish immune responses by secreting cytokines, including inhibitory IL-10 and TGF-β, which directly suppress cytotoxic T lymphocytes (CTLs) capability and promote tumor growth [20]. And MDSCs exert negative feedback by inhibiting T lymphocyte activity, releasing substances such as nitric oxide (NO) and reactive oxygen species (ROS) that hinder T cell function, and shifting macrophages to the M2-like phenotype, thereby enhancing immunosuppression and promoting tumor growth [21]. Similarly, certain types of neutrophils can also promote immune evasion through the secretion of IL-10 and TGF-β [22]. The immunosuppressive microenvironment is common in many malignant tumors, yet HCC shows unique characteristics when contrasted with breast cancer, pancreatic cancer, glioblastoma, and other types. The primary factors related to the initiation and progression of liver cancer include chronic viral hepatitis (HBV/HCV), cirrhosis, alcoholic liver disease, and aflatoxin exposure. These elements lead to extended chronic inflammation, resulting in irregular hepatocyte growth and tumor formation [23]. Unlike the hormone-driven immune evasion seen in breast cancer [24], the thick fibrosis typical of pancreatic cancer [25], and the blood-brain barrier isolation in glioblastoma [26], HCC fibrosis exhibits dynamic characteristics. In particular, the tumor core is mainly composed of Treg and MDSC, whereas the peripheral areas are rich in activated natural killer (NK) cells and CD8+ T cells. This “immune dual region” provides an opportunity for targeted matrix remodeling [27]. Additionally, ICIs show significant promise in treating HCC [28]. Building on this foundation, we are optimistic about the potential to develop micro-nano delivery systems capable of precisely responding to tumor region-specific signals. This advancement may offer a significant breakthrough in overcoming the current limitations of HCC immunotherapy.
The immunosuppressive microenvironment is crucial in the initiation, progression, and recurrence of HCC. The classification of tumors into “cold” and “hot” types in immunotherapy is determined by the presence of immune cell infiltration. Cold tumors, which have low levels of immune cell infiltration and limited immunogenicity. In contrast, hot tumors exhibit significant T lymphocyte infiltration, mainly consisting of CD8+ T cells, making them more susceptible to immune attacks [21]. Given the significant immunosuppressive signaling, HCC is frequently categorized as a “cold” tumor characterized by low immunogenicity, which results in a reduced responsiveness to immunotherapy. Therefore, in-depth understanding of the manner that tumor cells escape detection by the immune system highlights the necessity of converting cold tumors into hot tumors [29].
The liver's abundant vasculature and high metabolic function offer specific vascular and immune characteristics necessary for the development of micro-nano delivery systems. The blood vessels in HCC tumors are unusually dilated and more permeable, which enhances the possibility of passively targeting nanomaterials via the enhanced permeability and retention (EPR) effect. However, the fast pace of blood circulation and the phagocytic action of Kupffer cells cause NPs to be cleared rapidly. To improve delivery efficiency, these challenges require optimization using surface engineering techniques, like modifying with polyethylene glycol (PEG) to prolong circulation time and using galactose for targeted delivery to hepatocytes [30]. In contrast, micro-sized materials (1–100 µm) can obstruct tumor blood supply and facilitate sustained drug release via interventional embolization techniques, such as transarterial chemoembolization (TACE), by exploiting the anatomical characteristics of HCC, which predominantly receives its blood supply from the hepatic artery. Nonetheless, these materials may induce local hypoxia, leading to increased PD-L1 and VEGF, which might aggravate immunosuppression [31]. In breast cancer, the dynamic relationship between vascular materials and the immune system varies significantly because the EPR effect is absent in homogenized blood vessels [24]. In pancreatic cancer, the dense ECM hinders therapeutic penetration [32], while in glioblastoma, the blood-brain barrier restricts effective delivery [33]. Drawing on the aforementioned dynamic game characteristics of “vaso-material-immunity”, the design paradigm for micro-nanomaterials is transitioning from a singular functional focus to a precise alignment with the physiological and pathological attributes of HCC. By employing strategies such as surface engineering, size regulation, and environmentally responsive modifications, these material systems can effectively surmount the challenges posed by the liver's immune clearance mechanisms and the limitations of vascular delivery. Thus, this approach aids in the controlled release of immune-modulating drugs at specific times and locations. In the subsequent sections, we systematically describe typical materials, including organic-inorganic NPs, biomimetic nanovesicles, hydrogels, microspheres, and Pickering emulsions (Table S1 in Supporting information [34-64]), which play a pivotal role in counteracting the immunosuppressive microenvironment of HCC. This is accomplished by leveraging their biocompatibility, ability to integrate multiple functions, and potential for custom design. These materials not only improve drug delivery efficiency, surpassing the dosage limits of conventional therapies, but also implement a multidimensional synergistic strategy for immune regulation. The combined use of these materials has demonstrated considerable potential in improving the efficacy of immunotherapy for HCC.
NPs serve as significant drug delivery systems, generally measuring between 1 nm and 100 nm in diameter, possessing a significant surface-to-volume ratio and drug-loading capacity [65]. NPs can be classified into several categories: polymers, liposome NPs (LNPs), inorganic NPs (including gold, magnetic, and silica NPs), and biomimetic nanovesicles. In HCC immunotherapy, NPs can alter the TIME via multiple mechanisms, converting “cold” tumors into “hot” tumors (Fig. S2 in Supporting information). This reshaping of the TIME enhances drug targeting and therapeutic efficacy in a controlled manner.
Doxil, a liposomal doxorubicin (DOX) formulation, became the first NPs-based therapy for cancer treatment when it was approved in 1995 [66]. NPs have been recommended due to their capacity to improve antigen presentation efficiency, stimulate the immune system, and alter the TIME. The properties facilitate targeted delivery to tumor regions, enhance drug delivery to localized tumor sites, ensure prolonged drug release in vivo, and allow for efficient penetration through tumor vasculature and tissue barriers, thereby improving drug efficacy [67]. Active and passive targeting are two fundamental strategies employed in NPs delivery systems for drug delivery. In the context of uncontrolled tumor proliferation, tumor cells exhibit increased expression of VEGF to secure an adequate blood supply necessary for growth and continued proliferation. Excessive tumor angiogenesis results in enlarged and highly permeable blood vessels, which enhances the EPR effect [68]. Due to the incomplete and highly permeable nature of tumor vasculature, macromolecules and NPs can penetrate these vessels more easily [69]. Additionally, poor lymphatic drainage surrounding the tumor facilitates the prolonged retention of NPs at the tumor site. This mechanism allows unmodified NPs to accumulate in the tumor area, facilitating passive targeting. This characteristic improves the delivery capabilities of nanomedicine in immunotherapy by facilitating the transport of chemotherapeutic agents, ICIs, and other appropriately sized therapeutic agents to tumor sites, thus exerting antitumor effects. Passive targeting is relevant to multiple forms of nanocarriers, including polymeric NPs and liposomes. To enable selective recognition and targeting to tumor cells or protumor-associated cells, active targeting requires modifying the surfaces of NPs with particular targeting ligands, which might be antibodies, peptides, carbohydrates, or small compounds [70]. In HCC, prevalent targets include the epidermal growth factor receptor (EGFR), CD44, and PD-L1. NPs can be designed with ligands that selectively target tumor cells, thereby improving the accuracy of drug delivery, significantly elevating drug concentrations in tumor regions, reducing impacts on normal tissues, and increasing therapeutic efficacy [71]. In practice, passive and active targeting are commonly utilized in combination. Initially, NPs employ passive targeting to access tumor regions, subsequently utilizing active targeting to enhance their binding to specific cells or molecules. For example, NPs modified with anti-PD-L1 antibodies can passively accumulate in tumors and actively inhibit immune checkpoints, thereby improving the efficacy of immunotherapy [72]. Consequently, important considerations in NPs design include particle size, surface charge, and shape, which are essential for evaluating their delivery efficiency and therapeutic outcomes, as particle size directly influences passive targeting. Studies indicate that NPs ranging from approximately 5 nm to 100 nm exhibit an optimal EPR effect, facilitating their penetration into blood vessels and effective delivery of tumor antigens to lymph nodes. NPs with a size less than 5 nm can escape from blood vessels during circulation and be eliminated through renal metabolism. In contrast, NPs larger than 100 nm may have difficulty infiltrating tumor tissues and are more susceptible to phagocytosis and clearance by organs like the liver and spleen, thereby diminishing their antitumor effectiveness [73].
The surface charge of NPs also influences their interactions with cell membranes. Cell membranes generally possess a negative charge, which increases the likelihood of positively charged NPs binding to the membrane and undergoing endocytosis, thereby provoking stronger immune responses compared to neutral or negatively charged particles [74]. Additionally, positively charged NPs s typically demonstrate extended circulation times in the bloodstream due to their reduced susceptibility to capture by the reticuloendothelial system. Surface modifications, such as PEG, can reduce immune recognition and prolong the half-life of NPs in vivo [75]. However, excessively high positive charges may trigger autoimmune responses, consequently accelerating NPs clearance. Thus, it is essential to achieve a balanced surface charge design. The shape of NPs, alongside their size and surface charge, significantly influences the in vivo performance. Spherical particles are prevalent; however, recent studies indicate that non-spherical particles, such as rod- or disc-shaped forms, may demonstrate improved tumor penetration and retention times. Different immune cell types exhibit distinct tastes for particle shape, indicating that optimized shape design is crucial for improving targeting specificity [36,76]. Many studies have investigated immune therapies utilizing NPs delivery systems. Due to tumor immune evasion, conventional single-agent immunotherapies frequently exhibit restricted antitumor effectiveness and may result in adverse effects. As a result, combination immunotherapies utilizing NPs delivery systems have been created to incorporate various immunotherapeutic strategies. These systems seek to precisely target localized tumor regions and improve synergistic antitumor effects [77]. NPs delivery systems for immunotherapy in HCC can facilitate immune modulation by specifically targeting diverse immune cells within the HCC immune microenvironment. This strategy seeks to counteract the immunosuppressive TIME and improve the antitumor effectiveness. Polymeric NPs, particularly PEG, have become notable due to their superior biocompatibility, amphiphilic characteristics, and capacity to enhance the hydrophilicity of NPs. These properties render PEG an exceptional option for NPs design. Incorporating PEG allows NPs to evade rapid clearance and enhance tumor accumulation, thereby improving the therapeutic outcomes of HCC immunotherapy [78,79]. A study demonstrated that embedding the chemotherapeutic drug gemcitabine and antisense microRNA in PEGylated nanocarriers enhances cellular uptake and significantly improves antitumor effects in HCC [80]. Schmid's team developed polymer-based NPs loaded with immunotherapy drugs and antibodies targeting specific circulating T cells. Their research demonstrated that NPs bound to natural immune cells produced a more effective antitumor response compared to unbound drugs [81]. Yu et al. developed NPs composed of poly(lactic-co-glycolic acid) (PLGA), PEG, and aminoethyl anisamide (AEAA) for the co-delivery of icaritin and DOX. Icaritin triggers immunogenic cell death (ICD) through the enhancement of mitochondrial autophagy and apoptosis, and its combination with DOX shows synergistic effects at a low dose. The integrated delivery approach enhanced the treatment outcome of HCC, demonstrating a strong immune memory response. Furthermore, the combination of these NPs with a tyrosine kinase inhibitor significantly extended the survival time of mouse HCC models [82]. A separate study utilized LNPs for the co-delivery of miR-375 and DOX, with the objective of combining immunotherapy and addressing DOX resistance in HCC. The co-delivery approach effectively facilitated the transport of both agents to tumor cells and their subsequent release, thereby enhancing tumor cell apoptosis. This strategy demonstrated improved antitumor effectiveness in mouse HCC models [83].
Chitosan, recognized for its biodegradability and effective drug-release control capability, is widely employed in nanomedicine to improve therapeutic outcomes [84]. The stimulus-responsive characteristics of chitosan enable the release of drugs in response to internal or external triggers [85]. For example, a combination of chitosan and mesoporous silica NPs loaded with DOX has demonstrated sustained drug release under acidic pH conditions. This method demonstrated synergistic anti-cancer effects in HCC, decreasing multi-organ toxicity compared to free DOX, indicating great potential as an anti-cancer strategy [86]. Externally responsive nanomedicines, such as those utilizing pH, oxygen, photoacoustic effects, magnetism, and hyperthermia, have been developed for immunotherapy in HCC [87-91]. Khan et al. designed calcium carbonate NPs loaded with cisplatin and oleanolic acid to achieve a pH-dependent drug release. Combination therapy significantly reduces hepatotoxicity and induces apoptosis in liver tumor cells, exceeding the efficacy of free drug treatments [92]. For magnetism, Fe3O4 NPs are widely used as drug carriers in the treatment of HCC [93]. A study demonstrated that the combination of magnetic NPs and electromagnetic fields effectively induced apoptosis in liver tumor cells while minimally impacting normal liver tissue [94].
Sorafenib, a widely used therapeutic agent, has received approval for the treatment of advanced HCC due to its efficacy in prolonging patient survival. However, their limited targeting and efficacy remain significant challenges [95,96]. To address these shortcomings, researchers have designed NPs conjugated with monoclonal antibodies targeting glypican-3 (GPC3), a molecule specifically expressed in HCC. This system features controlled drug release, excellent targeting, high drug-loading capacity, safety, and stability [97]. A clinical trial utilizing this approach demonstrated that sorafenib-based NPs, when combined with TACE, significantly improved the therapeutic efficacy compared to TACE alone [98]. This study demonstrated the biocompatibility and selective targeting of liver tumor tissues, highlighting their unique therapeutic value in patients with HCC. A novel therapeutic approach was developed utilizing mesoporous ferric manganese NPs loaded with sorafenib (PMFNs@Sora) to replicate the activities of catalase and glutathione peroxidase, leading to apoptosis and ferroptosis to curb tumor development [99]. This form of therapy offers a promising approach with strong possibilities for clinical implementation.
In addition to the innovative NPs-based immune delivery systems discussed above, biomimetic strategies have emerged to enhance the practical performance of NPs. These strategies mimic the structures and functions of biological entities and offer versatile platforms for targeted drug delivery. Biomimetic NPs, which are designed to replicate natural biological molecules and structures such as cell membrane-derived NPs or vesicles, can achieve targeted activation and delivery of drugs [100]. By mimicking the natural cell membrane structure, cell membranes can be isolated and incorporated into NPs, or entire cells can be used as carriers to create biomimetic nanosystems. This approach enhances both biocompatibility and targeting properties, thereby improving the efficiency of drug delivery (Fig. S3 in Supporting information). Biomimetic NPs can simulate the characteristics of cell membranes and bind to specific receptors on the surface of tumor cells, enabling targeted drug delivery to HCC and reducing drug distribution in healthy tissues, which helps to minimize side effects [43]. Biomimetic NPs, with their multifunctional nature, act as drug carriers and potent instruments for influencing the TIME [101]. For instance, the design of tumor vaccines using cell membrane-derived NPs can be applied to boost the immunostimulatory and targeting effects of HCC immunotherapy [102]. Exosomes, nanosized vesicles secreted by cells, play a critical role in intercellular communication and are capable of transporting and transferring biomolecules, such as proteins, lipids, DNA, mRNA, and miRNA. Wang et al. designed stellate cell-derived exosomes loaded with therapeutic nucleic acids (miR-335–5p) for in vivo delivery. They found that miR-335–5p inhibited HCC cell proliferation and invasion, leading to tumor shrinkage in vivo. These results strongly support the potential of exosomes as novel drug delivery systems for HCC therapy [103]. Furthermore, biomimetic NPs coated with chimeric antigen receptor (CAR)-T cell membranes combined with photothermal therapy have shown high specificity in HCC treatment. This approach not only leverages the advantages of a drug delivery system but also harnesses the targeting capabilities of CAR-T cells, offering a promising strategy for HCC treatment [104].
To regulate the immune microenvironment in HCC, the design of targeted delivery systems must effectively navigate the challenges of tumor-specific recognition and avoid liver metabolism. Detailed consideration of liver and HCC targeting is vital. The liver, a key organ for metabolism and immune response, possesses unique physiological characteristics that frequently result in the unavoidable uptake of nanomaterials. Although physiological barriers within the liver, such as Kupffer cell phagocytosis and hepatic sinusoidal endothelial retention, contribute to the nonspecific accumulation of nanomaterials, active molecular targeting strategies, such as coupling with antigen glypican-3 (GPC-3) antibodies to recognize the HCC-specific GPC-3, can significantly enhance tumor uptake [97]. Bionic membrane technology enhances targeting efficiency by using NPs coated with tumor cell membranes, which show homologous targeting effects on HCC, leading to increased drug accumulation in tumor tissues. Additionally, when designing micro-nano materials, it is important to consider their liver clearance mechanisms to increase circulation duration and boost drug delivery efficiency. Improving the delivery of NPs to target tissues can be accomplished by modulating Kupffer cells' activity, such as by saturating their phagocytic capacity and preventing endocytosis [105]. In summary, a vital approach to increasing therapeutic success in HCC is optimizing the targeting of micro-nanomaterials. With the implementation of precise design and surface modification techniques, HCC can be targeted effectively, minimizing the impact on healthy liver tissue.
Hydrogels are three-dimensional polymer network structures composed of large amounts of water and crosslinked polymer networks. They are capable of absorbing substantial amounts of water and have a porous structure and strong hydrophilicity, which enable them to maintain excellent biological activity and robust mechanical properties [106]. Furthermore, hydrogels can be modified by physical and chemical means, attracting considerable attention in drug delivery systems, which often have significant side effects and may be metabolized before reaching the tumor tissue, thereby failing to exert optimal antitumor effects. In contrast to systemic drug delivery, local injection into the tumor and surrounding tissues can increase the concentration of therapeutic drugs in tumor-draining lymph nodes, enhance T-cell immune responses, and reduce systemic toxic side effects [107]. The application of hydrogels in HCC immunotherapy is widespread. The release rate of drugs can be precisely controlled by modifying the composition and structure of the hydrogels, allowing drugs to be released at specific times and locations to improve therapeutic outcomes. In addition, hydrogels increase the precision of targeting liver tumor cells, elevating the local drug concentration while lessening the impact on healthy cells. Hydrogels also aid in enhancing antigen presentation and ameliorating the immunosuppressive nature of the TME, these systems are unique among various drug delivery methods and can be classified as natural or synthetic depending on their origin [108]. Chitosan, alginate, and gelatin are typical biopolymers found in natural hydrogels, known for their excellent biocompatibility and ability to create stable biological environments in living organisms, thus minimizing immune rejection. However, natural hydrogels often have weak mechanical characteristics and lack adequate functionalization to overcome these constraints, and researchers typically adjust hydrogels to improve their suitability for personalized treatments [109]. Synthetic hydrogels provide the benefit of having adjustable physical properties and chemical structures tailored to specific requirements. Their mechanical strength and elasticity can be optimized, and they can be functionalized with various groups for more precise targeted delivery and controlled release [110]. Compared to traditional chemotherapy administered orally, hydrogels are typically delivered in injectable forms, allowing for local drug delivery. Injectability is also a specific feature of hydrogels for cancer therapy, and injectable hydrogels are usually prepared through physical or chemical crosslinking and injected or infused into the tumor tissues of patients. They can load multiple antigens and immune modulators to promote the in situ recruitment of immune cells, initiate specific immune responses [111], reduce drug circulation time in the body, minimize damage to healthy tissues, and shorten healing times [112]. Physical crosslinking is often achieved through non-covalent interactions such as ionic bonds, hydrogen bonds, hydrophobic interactions, π-bonds, and van der Waals forces. Chemical crosslinking, on the other hand, utilizes covalent bonds (click chemistry, Michael addition, and Schiff base formation). Injectable hydrogels can be further categorized into in situ and shear-thinning hydrogels. The former involves injecting the drug into the desired site, where it captures bioactive molecules or cells, whereas the latter is a material with lower viscosity during injection, which transforms into a gel at the tumor site through a sol-gel phase transition [113]. Both types of hydrogels can be formed through physical or chemical crosslinking. The resulting gel particles typically range in size to the nanoscale, allowing them to provide enhanced delivery capabilities owing to their smaller particle size [113]. Additionally, some hydrogels undergo sol-gel phase transitions in response to internal stimuli (such as pH and redox responses) and external stimuli (such as light, thermal, and magnetic responses). Hydrogels designed for HCC immunotherapy often adopt stimulus-responsive forms and serve as excellent drug reservoirs [114].
Specifically, hydrogels can load a variety of immune modulators, such as ICIs, cytokines, and drugs, to synergistically enhance the antitumor efficacy [115]. Hydrogels can be injected into the body or delivered via a catheter in TACE, which could locally deliver chemotherapeutic drugs to the tumor region [116]. As drug delivery carriers, hydrogels can also be loaded with both immunotherapeutic agents and metabolic regulators to achieve a combined therapeutic effect. Immunotherapy agents are directly delivered to enhance local immune responses, and the metabolic regulators adjust the tumor and further activate immune responses [50]. In a study, a chemical immunotherapy hydrogel consisting of sodium alginate (ALG) hydrogel loaded with albumin-bound paclitaxel (Nab-PTX) NPs and the immune stimulator R837 was used for local administration. These results demonstrated significant tumor cell-killing effects and inhibition of tumor growth. This combination induced ICD by exposing cells to immunogenic antigens. R837 promotes dendritic cell (DC) maturation and increases effector memory T cell populations, greatly enhancing antitumor efficacy in a mouse HCC model [117]. Wang et al. developed a prodrug hydrogel for the local delivery of ICIs) to enhance the immune response of the body against tumors. Their study showed that this carrier-free treatment system serves as a storage depot for camptothecin and PD-1 antibodies in tumors, generating immune-stimulating TIME and enhancing PD-1 blockade. In vivo results revealed that this combination of chemical and immunotherapy induced a strong and persistent systemic antitumor immune response, not only leading to tumor regression but also preventing tumor recurrence and metastasis [114]. The combination of NPs and hydrogels as delivery mediators has been widely applied for the treatment of HCC. Cheng et al. developed a single-dose injectable hydrogel nanovaccine containing three immune stimulators: a Toll-like receptor agonist (R848), a STING agonist, and an ICI [113]. Animal studies demonstrated that the single-dose hydrogel nanovaccine can reshape the TIME and improve tumor antigen accumulation in lymph nodes, converting “cold” tumors into “hot” tumors (Fig. S4A in Supporting information). Falcone et al. reported a drug-eluting shear-thinning hydrogel composed of gelatin and nanoclay for the delivery of both chemotherapeutic and immunotherapeutic agents for HCC treatment [116]. The system was delivered via a catheter for intravascular anti-tumor therapy. In a mouse liver tumor model, remarkable results were observed, with increased tumor cell apoptosis and enhanced cytotoxic T cell infiltration following the combined delivery of DOX and PD-1 antibody, demonstrating clinical relevance (Fig. S4B in Supporting information). Song et al. developed an injectable immune-regulating multi-domain nanogel (iGel) formed through electrostatic interactions between negatively charged multi-nanodomain vesicles and positively charged nanoliposomes. Immunomodulatory drugs are encapsulated within nanoliposomes, and the gel structure temporarily dissociates during injection and is subsequently reassembled at the treatment site. The experimental results showed that iGel could remodel immunosuppressive TIME. Flow cytometry analysis indicated a significant increase in CD8+ T cells and interferon-γ (IFN-γ) secretion in the tumor and spleen [118]. The combination of immune and metabolic therapies for cancer treatment is gaining popularity. One study reported in situ hydrogel-mediated chemical-immunometabolic therapy, in which supramolecular hydrogels were injected peritumorally to release DOX and kynurenine-3-monooxygenase (Kyn) inhibitors [50]. This dual release induces immunogenic tumor cell death and disrupts immunosuppressive pathways. This synergistic approach enhances effector T cell infiltration and the activation of antigen-presenting cells, thereby promoting tumor immunogenicity and activating systemic anti-tumor immunity (Fig. S4C in Supporting information). These NPs represent an excellent drug delivery system, and when combined with the advantageous properties of hydrogels, they form stable nanocomposite hydrogels for drug delivery systems [119].
Studies have demonstrated that nanocomposite hydrogels have significant efficacy in HCC combined therapy. Peng et al. proposed a composite hydrogel based on self-assembly strategy, which is composed of the chemotherapy drug raltitrexed, kaempferol, and tantalum NPs [120]. Specifically, without the need for external chemical cross-linkers, a stable hydrogel structure can be achieved through simple ultrasound. RKT@gel can achieve sustained and stable drug release at the tumor site, avoiding the problem of excessive drug release of traditional embolic materials. The immune response was significantly activated through the ICD effect induced by RKT@gel. The study found that RKT@gel can activate DCs and enhance the immune surveillance and killing of tumors through major histocompatibility complex class Ⅰ (MHC-Ⅰ)-mediated anti-tumor immune recognition. This discovery provides a new breakthrough for immunotherapy of HCC. The tantalum NPs of RKT@gel not only serve as X-ray contrast agents to guide precision treatment but also enhance the sensitivity of tumors to radiation during radiotherapy, thereby improving the therapeutic effect of HCC (Fig. S4D in Supporting information). Zhu et al. synthesized a block copolymer composed of PEG and polyglutamic acid to encapsulate two monoclonal antibody drugs. The synthesis process involved precipitation polymerization and the formation of nanoscale core-shell structures. In addition, magnesium-calcium carbonate NPs have been used to load monoclonal antibody drugs to enhance their stability. The final product was a fibrin hydrogel. This hydrogel prolonged and enhanced the impact of immunotherapy while controlling the release of components within the synthetic hydrogel, significantly improving the prevention of postoperative wound bleeding and greatly enhancing the safety of HCC resection surgery [110]. Ascites caused by advanced HCC is a complex clinical issue, and there are currently no effective treatments. One study designed an injectable hydrogel drug delivery system composed of chitosan hydrochloride and oxidized dextran, which was loaded with sulfasalazine (SSZ), a Food and Drug Administration (FDA)-approved drug that induces ferroptosis. This hydrogel effectively activated anti-tumor immune responses and killed tumor cells. In both in vitro and in vivo experiments, the hydrogel induced macrophage repolarization to an M1-like phenotype, promoted the maturation and activation of DCs, and when used in combination with PD-1 immunotherapy, resulted in at least a 50% reduction in ascites and long-term tumor immune memory [121]. Hydrogels combined with photodynamic therapy (PDT) offer a more effective way to eliminate tumor cells and exert stronger immune effects. Meng et al. designed a light-triggered in situ gel system based on a hydrogel responsive to external stimuli using photosensitizer-modified catalase and poly(ethylene glycol) diacrylate (PEGDA) as the polymer matrix. Immunoadjuvant NPs were further introduced into the system to trigger a powerful anti-tumor immune response after PDT. This gel-based PDT therapy, combined with checkpoint blockade targeting CTL antigens, not only provides a distant effect to inhibit tumor growth but also offers effective long-term immune memory protection, preventing tumors from re-challenging [122]. Hydrogel-based cytokine therapy is a feasible approach for cancer treatment. Li et al. prepared a hydrogel that adsorbed IL-6 through subcutaneous injection and conjugated IL-6-specific antibodies to a thermosensitive hydrogel made of poly(N-isopropylacrylamide-methacrylic acid). This approach was designed to prevent CRS caused by CAR-T cell therapy. The study found that it significantly reduced IL-6 levels during CRS while maintaining the anti-tumor efficacy of the therapy [123].
Microspheres are widely used as drug carrier platforms in drug delivery systems for HCC. They are primarily applied in TACE, where they load therapeutic drugs to reach the local tumor area and achieve precise drug release. This not only improves HCC treatment efficacy but also significantly reduces damage to normal liver tissue and other healthy organs. TACE has become the standard treatment for unresectable HCC, and conventional transarterial chemoembolization (cTACE) mixes chemotherapy drugs with lipiodol, an FDA-approved interventional agent [124,125]. Compared with cTACE, drug-eluting beads (DEB-TACE) are good embolic agents and drug delivery carriers, enabling continuous and stable drug release at the tumor site. This results in higher local tumor drug concentrations and significantly reduces drug-related and liver toxicity [126]. Additionally, because DEB-TACE does not require the use of Lipiodol, it reduces the occurrence of Lipiodol retention issues [127]. In the development of new microsphere materials, biodegradable microspheres, such as gel sponges and calcium alginate microspheres, have been widely used for vascular embolization, effectively enhancing their biocompatibility in the body. These embolization agents are produced in various sizes to obstruct the vascular system [128]. Moreover, surface structure modification of these microspheres can boost their functionality and targeting ability, allowing for more targeted drug delivery to tumor sites [129]. Additionally, radioactive microspheres and drug-eluting beads (DEBs) are present. Y-90 microspheres, which are radioactive, can vary from having a resin-like to glass-like composition and contain isotopes, measuring under 300 µm in diameter, utilizing localized radiation to destroy tumor cells, and serving an embolization role. Commonly used DEB microspheres, such as Hepasphere, are primarily made from polyvinyl alcohol (PVA) and used to load drugs such as DOX and irinotecan [130]. These non-absorbable, small-sized HepaSphere microspheres have been in use for years and can embolize even more remote sections of tumors, and chemotherapy drugs are released in a controlled manner over an extended period, leading to reduced systemic toxicity. Clinical studies conducted abroad have demonstrated the good anti-tumor effects and biological safety of these microspheres [131,132]. In a single-center, prospective randomized controlled trial (TRACE), treatment with Y-90 microspheres was compared with DEBs loaded with DOX. The study found that both treatments had similar biological safety; however, the Y-90 microspheres led to a higher tumor control rate and significantly extended patient survival [133]. Currently available microspheres include Y-90 resin microspheres (Sir-Spheres®), Y-90 glass microspheres (Therasphere®), and Ho-PLLA microspheres (QuiremSpheres®) [134]. Compared to standard chemotherapy or radiotherapy, the introduction of microspheres for different forms of HCC embolization helps reduce systemic adverse effects, as microspheres can selectively reach tumors via the hepatic artery while preserving most of the healthy liver tissue [135]. DOX is a chemotherapeutic drug commonly used for embolization therapy in HCC. Zhong et al. designed a novel microsphere composed of sodium alginate (ALG) shell and methacrylated gelatin (GelMA) loaded with DOX and a liver regeneration enhancer (ALR). These dual-drug-loaded microspheres exhibited significant postoperative tumor-killing ability and promoted liver regeneration [136]. Chen et al. developed multifunctional PVA/hyaluronic acid (HA)-based microspheres (PT/DOX-MS) co-loaded with DOX and the hypoxia inducible factor-2 alpha (HIF-2α) inhibitor PT-2385 to enhance TACE therapy. Both in vitro and in vivo experiments showed that these microspheres blocked the G2 phase of HCC cells, induced apoptosis, inhibited tumor angiogenesis, and improved the hypoxic status. The combination of chemotherapy and embolization significantly enhances the therapeutic effects in HCC treatment [137]. Li et al. prepared microspheres loaded with tirapazamine (TPZ), a chemotherapeutic embolic agent. Their results showed that this approach significantly outperformed chemotherapy and arterial embolization in inducing acute tumor hypoxia, tumor apoptosis, necrosis, and safety. In a rabbit VX2 HCC model, the microspheres enhanced synergistic antitumor effects and demonstrated great potential for clinical translation [138]. The hypoxia-responsive pharmacological properties of TPZ and the microenvironmental features of TACE in liver cancer are both fully used in the application of TPZ in TACE. Recent research demonstrated the combination of TPZ and sorafenib can greatly increase the effectiveness of TACE therapy for advanced HCC [96]. Another study synthesized a new type of embolic agent, calcium carbonate-encapsulated alginate microspheres (CaCO3-ALGMSs), which not only neutralized tumor pH but also enhanced tumor-infiltrating effector T cells when combined with TACE treatment. This approach reverses the immune microenvironment, further boosting antitumor effects [139]. To overcome the limitations of traditional TACE therapy, such as unstable emulsions causing rapid dissociation and insufficient local drug concentrations, Zheng et al. designed biodegradable microspheres (BILMs) loaded with idarubicin (IDA-MS). In mouse HCC models and rabbit tumor models, drug-loaded microspheres resulted in significant tumor shrinkage compared to the use of drugs alone, and TACE combination therapy significantly enhanced sensitivity to anti-PD1 immunotherapy [140]. Additionally, a novel magnetic mesoporous embolic microsphere was reported that could simultaneously load DOX and block blood vessels, with the effect observed through magnetic resonance imaging (MRI). Microspheres made from magnetic polystyrene-iron and mesoporous organic silica particles were used in a VX2 rabbit liver tumor model. The combination of TACE treatment with these microspheres completely blocked the tumor blood supply, offering a new approach for enhancing TACE therapy and post-treatment evaluation [141]. Especially in immune embolization therapy combined with magnetic hyperthermia (MHT) effects, the application of microspheres not only improves the precision and efficacy of the treatment but also significantly enhances the anti-tumor immune response. Yang’s team developed liquid metal microspheres with eddy current heating effects and proposed an effective strategy for enhancing cancer immunotherapy using MHT combined with transarterial embolization (TAE) to treat HCC [142]. Precise heating of the tumor was achieved through the magnetic heating effect, and the uniform liquid metal microspheres (LM MSs) obtained via microfluidic technology exhibited strong eddy current effects, making them suitable for use as MHT and TAE drugs for effective cancer treatment. This approach promotes immune cell infiltration and further strengthens the immune response by inhibiting the growth of distant tumors. Additionally, it highlighted the significant potential of combining MHT with TAE for the effective treatment of large in situ liver tumors (Fig. S5 in Supporting information). In addition, 131I, a commonly used radioactive isotope, has been used to develop stable multifunctional embolic agents. When loaded with DOX, these agents allow for low-dose embolization combined with simultaneous HCC treatment, showing significant clinical potential [58].
In the treatment of advanced HCC, iodized oil lipid-based chemotherapy emulsion remains the key choice for TACE embolic material. However, as previously mentioned, conventional TACE treatment often faces the risk of tumor recurrence and metastasis, which has driven researchers to explore new strategies to enhance its therapeutic efficacy. In recent years, the emergence of nano- and micro-material-assisted emulsions has provided a new perspective for TACE treatment, particularly showing great potential in activating anti-tumor immune responses in HCC [106]. NPs emulsions can be loaded with immunomodulators and chemotherapeutic agents, achieving precise drug delivery and regulation through their unique physicochemical properties. The emulsion was initially delivered to the hepatic artery, supplying blood to the tumor during TACE treatment. Subsequently, it can slowly release drug in the localized tumor area, effectively blocking blood supply while stimulating the body's immune system to generate anti-tumor immune responses. In addition, micro-nanomaterials-assisted emulsions also play a role in improving the TIME. These emulsions create a more favorable microenvironment for immune cell infiltration and functional activity by modulating factors such as angiogenesis, hypoxia, and immune suppression within the tumor. Pickering emulsions, a novel type of emulsion that uses solid NPs as emulsifiers instead of organic surfactants, demonstrate strong capabilities in encapsulating various water-soluble agents for different applications [143]. Wang et al. developed a stable water-in-oil iodized oil Pickering emulsion (L-Arg@CaPL) using calcium phosphate NPs (CaP NPs) as stabilizers to encapsulate L-arginine (L-Arg) to regulate T cell metabolism [60]. The results showed that the synthesized emulsion exhibited good stability and could regulate the acidic pH of the tumor by neutralizing H+ via CaP NPs, thereby reversing the immunosuppressive TIME (Fig. S6A in Supporting information). Besides, it continuously releases L-Arg to modulate T cell metabolism, promoting the activation of CD8+ T cells and enhancing their tumor-killing effect. In a subcutaneous H22 mouse HCC model, L-Arg@CaPL significantly inhibited tumor growth and prolonged animal survival. In the N1S1 rat orthotopic HCC model, L-Arg@CaPL, when used in TACE treatment, significantly suppressed tumor progression, showing superior efficacy compared with TACE treatment alone. In a similar study, Liang et al. developed a Rhein-based Pickering emulsion (R-EM), stabilized by self-assembled rhein nanogels for use in TACE treatment [62]. Rhein, a natural small compound [144], which can assemble into hydrogel with nanofiber structure [145]. This self-assembled material has shown good therapeutic effect in antimicrobial therapy [146]. In this work, the authors identified Rhein as a potential glycolysis metabolism inhibitor and immune activation inducer, which enhances tumor sensitivity to TACE. Compared with the traditional triple-lumen catheter mixing method, multimodal imaging showed that R-EM significantly enhanced local drug retention and tumor suppression. In animal models, the R-EM emulsion demonstrated efficient embolization capacity and sustained drug-release properties. The Rhein-mediated synergistic immune embolization strategy not only achieved effective embolization but also effectively activated anti-tumor immune responses by inducing ICD, activating DCs, and presenting MHC-I molecules to CD8+ T cells (Fig. S6B in Supporting information). The study by Ye et al. utilized an oil-in-water attractive Pickering latex gel (APEG) for delivering oxaliplatin and lactate dehydrogenase A inhibitors, which resulted in enhanced delivery efficiency and anti-tumor therapeutic efficacy. The study demonstrated a notable anti-tumor impact on models of HCC. Moreover, flow cytometry analysis verified the activation of the TIME in HCC [147]. Likewise, Zhang et al. prepared a calcium phosphate NPs-stabilized iodized oil Pickering emulsion (CaP-LPE) to encapsulate the clinically approved vascular-disrupting agent CA4P. Compared with traditional iodized oil emulsions, CA4P-loaded CaP-LPE (CCaP-LPE) exhibited better emulsion stability and pH-responsive drug release behavior. CCaP-LPE can reverse the immunosuppressive TIME by disrupting tumor vasculature and neutralizing tumor acidity, thereby increasing CD8+ T cell infiltration and reducing the proportion of immunosuppressive cells [61]. Xia et al. developed a novel drug-loaded iodized oil emulsion (ICN-LPE) stabilized by iron-doped carbon nanoperoxidase (ICN) to address the issue of iodized oil-water separation. ICN can catalyze the generation of ROS while depleting intracellular glutathione (GSH), thereby inducing tumor cell death. In vitro experiments demonstrated that ICN exhibited excellent peroxidase catalytic activity and blood compatibility, while ICN-LPE was able to stably release chemotherapeutic drugs over 48 h. In the New Zealand rabbit VX2 liver tumor model, ICN-LPE significantly inhibited tumor growth, showing promising anti-tumor efficacy [148]. In the future, with continuous advancements in materials science and immunology, micro-nanomaterials-assisted emulsions are expected to become an important adjunct in TACE treatment for HCC, offering more effective and personalized treatment options for patients with advanced HCC.
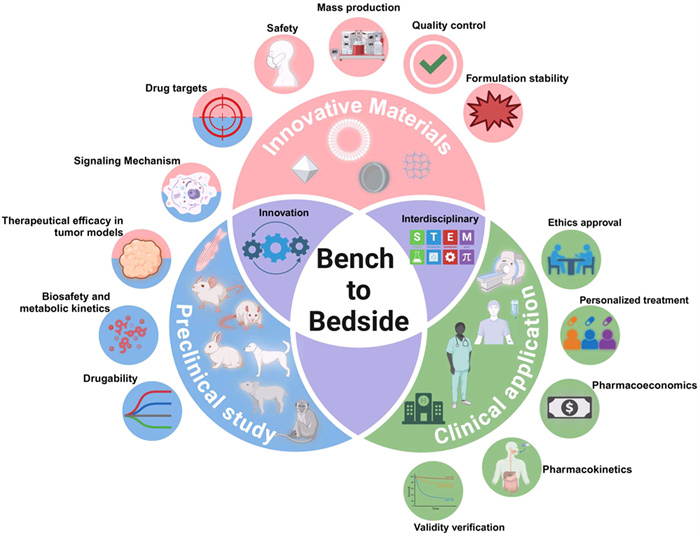
Targeted therapies and immunotherapy have been hot research topics in the clinical translation of HCC treatment. One of the first-line therapeutic agents, the multitargeted kinase inhibitor sorafenib, has been widely used, but the clinical translation rate of a single agent is poor [149]. Drugs such as regorafenib and apatinib are used as second-line therapeutic agents [150]. The implementation of neoadjuvant therapy for HCC based on immunotherapy has also shown initial success. Clinical studies of apatinib in combination with a carryilizumab monoclonal antibody have been reported to be effective in alleviating postoperative pathologic features in phase Ⅱ clinical trials [151]. Nanomaterials can be targeted to specific areas of the disease, thereby reducing the off-target effects of drugs. Micro-nanomaterials designed for delivery systems provide dual functions in liver cancer therapy. Passive carriers like liposomes, polymer NPs, and embolic microspheres greatly improve drug bioavailability and minimize systemic toxicity by accurately delivering chemotherapy drugs or immunomodulators, such as PD-1 antibodies and miRNAs [103,116]. However, their effectiveness depends on the activity of the drugs they assist. On the other hand, active immunomodulators, exemplified by bionic membrane NPs, MnO2 nanosheets, and stimulation-responsive hydrogels, can directly modulate the TIME through material properties such as hypoxia response, immune escape, and metabolic regulation. The materials lead to ICD, reverse M2-type macrophage polarization, or activate DC maturation, resulting in a synergistic “delivery-immunity” effect [60,117]. For instance, liquid metal microspheres, in conjunction with magnetothermal effects, can simultaneously obstruct tumor blood supply and promote T cell infiltration [142]. However, the preparation and synthesis of nanomaterials are complex, and after entering the organism, they sometimes produce toxic effects [152]. Their potential immunogenicity may activate the body's autoimmunity and induce an inflammatory response in the body, which can cause adverse response behavior. For example, they may be recognized by the body as foreign antigens to activate the complement pathway, the drug will be cleared by the liver and spleen, thus losing the anti-tumor effect. Furthermore, if the body's immune response is overactivated, serious complications may occur, such as allergic reactions. Therefore, in the clinical translation of nanomaterials, it is necessary to continue to innovate the development of nanotechnology, optimize the selection of materials and the process of preparation, improve the biosafety of nanomaterials, and develop more novel nanomedicines and carriers with excellent properties [153], and the biosafety of the materials is a prerequisite for the clinical translation. prerequisite for clinical translation and to observe long-term immunofunctionality and host tissue response when acting in vivo [154]. Hydrogels, in the field of HCC treatment, are mainly applied to fabricate stimuli-responsive hydrogels to deliver various immunotherapeutic agents, including adriamycin, paclitaxel, and cisplatin chemotherapeutic drugs, to tumor tissues [155], to achieve the release of therapeutic drugs in the localized area of the tumor and to reduce the systemic toxicity of drugs that cause serious side effects, the first of which is whether the hydrogel can be applied easily [119]. Although some hydrogels can be administered by intravenous injection, there are still many that cannot be injected, and their application in the clinic may be limited [156]. Although a large number of studies have validated the effect of these materials in treating tumors by using animal models, and it is also possible to assess the biocompatibility of these materials in the short term, trials in humans need to consider the long-term safety and biocompatibility effects; therefore, further consideration should be given to more comprehensive studies in large human animal models, and the synthesis of the materials and whether they can be mass-produced should be refined. In human clinical treatment plans, it is important to consider whether the treatment costs are prohibitively high, whether the patient has the financial capacity to afford the treatment, how to implement a personalized, patient-specific approach, and how to achieve better prognosis outcomes (Fig. 1).
Micro-nanomaterials-based delivery systems, including NPs and hydrogels, are changing the landscape of drug delivery for HCC by boosting bioavailability, facilitating controlled release, and merging various therapeutic approaches. Using strategies like the co-delivery of ICIs, they improve targeting precision, reduce systemic toxicity, and counteract drug resistance [7]. For instance, NPs with ligands specific to HCC enhance targeting of tumors, whereas hydrogels enable prolonged drug release in fibrotic settings [157]. Nonetheless, increasing the production of these advanced materials is difficult because it requires precise control over their properties and involves complex synthesis processes. Moreover, nanomaterials are susceptible to immune clearance processes like Kupffer cell phagocytosis, which can lead to unintended distribution in the body, potentially causing off-target effects or reduced therapeutic effectiveness [158]. The challenges of maintaining compatibility and stability of active pharmaceutical ingredients (APIs), the vital functional elements of drugs, are heightened for biologics such as mRNA or antibodies, which demand exact encapsulation conditions to preserve their activity. Additionally, the dynamic and heterogeneous TIME requires materials that can adjust in real-time to immunosuppressive signals [159]. Future progress in this field should focus on the development of smart material designs, including stimuli-responsive NPs that are activated by TIME-specific cues, such as ROS, pH, or matrix metalloproteinases (MMPs) [160]. Moreover, it is crucial to explore combinatorial strategies that integrate nanocarriers with emerging therapies, such as CAR-T cells and oncolytic viruses [161]. Addressing scalability and safety issues requires cost-effective manufacturing approaches, including AI-driven synthesis, biodegradable polymers, and standardized frameworks for preclinical-to-clinical evaluation. By utilizing multi-omics profiling techniques like spatial metabolomics and single-cell sequencing, precision medicine will advance patient stratification for customized nanotherapy [162]. Global cooperation is also necessary to synchronize regulatory standards and hasten translational advancements.
The treatment of HCC has been greatly changed by immunotherapy, especially with the use of ICIs. However, obstacles such as the restrictions of focusing on single molecules, adaptive resistance mechanisms, and unintended toxicities continue to be significant barriers. Micro-nanoengineered delivery systems could lead to a significant change in therapeutic approaches by boosting precision, lowering adverse effects, and transforming the immunosuppressive TIME. Preclinical innovations in biomimetic nanovesicles, injectable hydrogels, and interventional embolization microspheres reveal their capacity to collectively enhance apoptosis, ferroptosis, and immune activation. However, for true human treatments, a more rigorous and comprehensive evaluation is required, considering the significant individual differences in cancer patients, such as treatment doses, regimen choices, treatment costs, safety, and efficacy. As precision medicine continues to evolve, HCC treatment will focus on personalized approaches. With the help of omics technologies, it will be possible to more accurately identify the characteristics of a patient's tumor and design treatment methods based on specific targets, thus enabling individualized therapy. Additionally, future research should explore the combined application of novel drug delivery technologies to enhance treatment effectiveness, and new materials must be developed to meet the requirements of complex systems. In clinical trials, a broader patient population should be considered to ensure the reliability of research results. In particular, regarding the immunosuppressive TIME in HCC, further research is needed to uncover new targets and treatment pathways. Finally, in the context of global integration, the advancement of cancer treatment requires interdisciplinary collaboration and global resource-sharing. International cooperation can accelerate the development of novel therapies. We predict that novel drug delivery systems will provide more effective strategies for tumor treatment in the future.
In summary, micro-nanomaterials not only enhance the efficiency of drug delivery for HCC but also remodel the immunosuppressive TME. These materials exert comprehensive mechanistic effects across the whole immune activation cascade, including tumor antigen release, antigen presentation and processing, cytotoxic T cell activation and infiltration, as well as immune recognition and killing. Their synergistic application with multimodal therapies demonstrates transformative potential in overcoming treatment resistance and amplifying therapeutic efficacy. The continued advancement of these technologies is poised to drive innovation in HCC drug development and inspire novel clinical strategies for personalized immunotherapy.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Mengmeng Miao: Writing – original draft, Visualization, Resources, Investigation. Yisheng Peng: Writing – original draft, Conceptualization. Hui Liu: Writing – original draft. Hu Chen: Visualization. Xu Cheng: Resources. Shangqing Chen: Resources. Kaifei Yan: Resources. Hongwei Cheng: Writing – review & editing, Writing – original draft, Visualization, Supervision, Funding acquisition, Conceptualization. Gang Liu: Writing – review & editing, Supervision, Funding acquisition, Conceptualization.
This work was supported by the Major State Basic Research Development Program of China (No. 2023YFB3810000), the National Natural Science Foundation of China (NSFC, Nos. U22A20333, 81925019, U1705281, and 82202330), the Fundamental Research Funds for the Central Universities (No. 20720200019), the Program for New Century Excellent Talents in University, China (No. NCET-13–0502), and China Postdoctoral Science Foundation (No. 2024M763915). We thank BioRender.com for creating the schematic illustration.
Supplementary material associated with this article can be found, in the online version, at doi:
Z.J. Brown, D.I. Tsilimigras, S.M. Ruff, et al., JAMA Surg. 158 (2023) 410–420. doi: 10.1001/jamasurg.2022.7989
G. Brar, T.F. Greten, B.I. Graubard, et al., Hepatol. Commun. 4 (2020) 1541–1551. doi: 10.1002/hep4.1564
M. Yilma, R. Xu, V. Saxena, et al., JAMA Netw. Open. 7 (2024) e2435066. doi: 10.1001/jamanetworkopen.2024.35066
R. Donne, A. Lujambio, Hepatology 77 (2023) 1773–1796. doi: 10.1002/hep.32740
A. Ribas, J.D. Wolchok, Science 359 (2018) 1350–1355. doi: 10.1126/science.aar4060
R.S. Finn, S. Qin, M. Ikeda, et al., N. Engl. J. Med. 382 (2020) 1894–1905. doi: 10.1056/nejmoa1915745
M. Yi, X. Zheng, M. Niu, et al., Mol. Cancer 21 (2022) 28. doi: 10.1186/s12943-021-01489-2
F. Qu, Y. Zhou, S. Wu, Br. J. Cancer 130 (2024) 165–175. doi: 10.1038/s41416-023-02482-w
E. Batlle, J. Massagué, Immunity 50 (2019) 924–940. doi: 10.1016/j.immuni.2019.03.024
W. Ngwa, O.C. Irabor, J.D. Schoenfeld, et al., Nat. Rev. Cancer 18 (2018) 313–322. doi: 10.1038/nrc.2018.6
E.W. Weber, M.V. Maus, C.L. Mackall, Cell 181 (2020) 46–62. doi: 10.1016/j.cell.2020.03.001
K.E. Yost, H.Y. Chang, A.T. Satpathy, Science 372 (2021) 130–131. doi: 10.1126/science.abd1329
J. Galon, D. Bruni, Nat. Rev. Drug Discov. 18 (2019) 197–218. doi: 10.1038/s41573-018-0007-y
K.E. De Visser, J.A. Joyce, Cancer Cell 41 (2023) 374–403. doi: 10.1016/j.ccell.2023.02.016
Z. Sas, E. Cendrowicz, I. Weinhäuser, E.T. AL, Int. J. Mol. Sci. 23 (2022) 3778. doi: 10.3390/ijms23073778
K.J. Hiam-Galvez, B.M. Allen, M.H. Spitzer, Nat. Rev. Cancer 21 (2021) 345–359. doi: 10.1038/s41568-021-00347-z
L.B. Kennedy, A.K.S. Salama, CA. Cancer. J. Clin. 70 (2020) 86–104. doi: 10.3322/caac.21596
J.P. Böttcher, E. Bonavita, P. Chakravarty, et al., Cell 172 (2018) 1022–1037. doi: 10.1016/j.cell.2018.01.004
L. Kaps, D. Schuppan, Cells 9 (2020) 2027. doi: 10.3390/cells9092027
Y. Zhao, J. Chen, M. Andreatta, et al., Nat. Biotechnol. 42 (2024) 1693–1704. doi: 10.1038/s41587-023-02060-8
M. Binnewies, E.W. Roberts, K. Kersten, et al., Nat. Med. 24 (2018) 541–550. doi: 10.1038/s41591-018-0014-x
J. Xie, Q. Li, F. Haesebrouck, et al., Trends. Biotechnol. 40 (2022) 1173–1194. doi: 10.1016/j.tibtech.2022.03.005
P. Kubes, C. Jenne, Annu. Rev. Immunol. 36 (2018) 247–277. doi: 10.1146/annurev-immunol-051116-052415
S.S. Onkar, N.M. Carleton, P.C. Lucas, et al., Cancer Discov. 13 (2023) 23–40. doi: 10.1158/2159-8290.cd-22-0475
A.S. Bear, R.H. Vonderheide, M.H. O’Hara, Cancer Cell 38 (2020) 788–802. doi: 10.1016/j.ccell.2020.08.004
J.R.D. Pearson, S. Cuzzubbo, S. McArthur, et al., Front. Immunol. 11 (2020) 582106. doi: 10.3389/fimmu.2020.582106
K. Cheng, N. Cai, J. Zhu, et al., Cancer Commun. 42 (2022) 1112–1140. doi: 10.1002/cac2.12345
M. Pinter, B. Scheiner, D.J. Pinato, Lancet Gastroenterol. Hepatol. 8 (2023) 760–770. doi: 10.1016/S2468-1253(23)00147-4
J.M. Llovet, F. Castet, M. Heikenwalder, et al., Nat. Rev. Clin. Oncol. 19 (2022) 151–172. doi: 10.1038/s41571-021-00573-2
R. Liu, C. Luo, Z. Pang, et al., Chin. Chem. Lett. 34 (2023) 107518. doi: 10.1016/j.cclet.2022.05.032
H. Chen, H. Cheng, W. Wu, et al., Chin. Chem. Lett. 31 (2020) 1375–1381. doi: 10.1016/j.cclet.2020.03.024
H.Y. Tanaka, M.R. Kano, Cancer Sci. 109 (2018) 2085–2092. doi: 10.1111/cas.13630
O. van Tellingen, B. Yetkin-Arik, M.C. de Gooijer, et al., Drug Resist. Updat. 19 (2015) 1–12.
J. Wang, Y. Qian, L. Xu, et al., Mater. Sci. Eng. C: Mater. Biol. Appl. 117 (2020) 111261. doi: 10.1016/j.msec.2020.111261
X. Hou, T. Zaks, R. Langer, et al., Nat. Rev. Mater. 6 (2021) 1078–1094. doi: 10.1038/s41578-021-00358-0
R. Böttger, G. Pauli, P.-H. Chao, et al., Adv. Drug. Deliv. Rev. 154-155 (2020) 79–101. doi: 10.1016/j.addr.2020.06.017
J. Beik, M. Khateri, Z. Khosravi, et al., Coord. Chem. Rev. 387 (2019) 299–324. doi: 10.1016/j.ccr.2019.02.025
M.T. Yassin, F.O. Al-Otibi, S.A. Al-Sahli, et al., Cancers 16 (2024) 4234. doi: 10.3390/cancers16244234
S. Zhao, X. Yu, Y. Qian, et al., Theranostics 10 (2020) 6278–6309. doi: 10.7150/thno.42564
A.M. Abu-Dief, M. Alsehli, A. Al-Enizi, et al., Curr. Drug. Deliv. 19 (2022) 436–450. doi: 10.2174/1567201818666210708123007
H. Wu, X.F. Xu, J.Q. Zhu, et al., Front. Bioeng. Biotechnol. 9 (2021) 695635. doi: 10.3389/fbioe.2021.695635
H. Zhang, A. Grippin, M. Sun, et al., J. Control. Release 375 (2024) 712–732. doi: 10.1016/j.jconrel.2024.09.037
C. Marar, B. Starich, D. Wirtz, Nat. Immunol. 22 (2021) 560–570. doi: 10.1038/s41590-021-00899-0
H. Zhu, H. Sun, J. Dai, et al., Int. J. Biol. Macromol. 282 (2024) 137047. doi: 10.1016/j.ijbiomac.2024.137047
Z. Tang, L. Deng, J. Zhang, et al., Research 7 (2024) 0477. doi: 10.34133/research.0477
X. Liang, L. Ding, J. Ma, et al., Adv. Healthc. Mater. 13 (2024) e2400841. doi: 10.1002/adhm.202400841
X. Liang, C. Huang, H. Liu, et al., Chin. Chem. Lett. 35 (2024) 109442. doi: 10.1016/j.cclet.2023.109442
B. Zhao, B. Zhou, K. Shi, et al., Cancer Sci. 112 (2021) 2481–2492. doi: 10.1111/cas.14903
Y. Jiang, X. Meng, Z. Wu, et al., Carbohydr. Polym. 144 (2016) 245–253. doi: 10.1016/j.carbpol.2016.02.059
B. Wang, J. Chen, J.S. Caserto, et al., Nat. Commun. 13 (2022) 3821. doi: 10.1038/s41467-022-31579-8
P.V. Londhe, M.V. Londhe, A.B. Salunkhe, et al., Coordin. Chem. Rev. 522 (2025) 216228. doi: 10.1016/j.ccr.2024.216228
P. Pan, D. Svirskis, S.W.P. Rees, et al., J. Control. Release 338 (2021) 446–461. doi: 10.1016/j.jconrel.2021.08.053
T.J. Yeingst, J.H. Arrizabalaga, D.J. Hayes, Gels 8 (2022) 554. doi: 10.3390/gels8090554
Y.T. Liao, C.H. Liu, J. Yu, et al., Int. J. Nanomedicine 9 (2014) 2767–2778.
S.H. Lee, C.Y. Lin, Y.C. Hsu, et al., Cancer Res. Treat. 52 (2020) 24–30. doi: 10.4143/crt.2019.018
K. Malagari, H. Moschouris, T. Kiakidis, et al., Cardiovasc. Intervent. Radiol. 42 (2019) 1551–1562. doi: 10.1007/s00270-019-02260-3
J.R. Kallini, A. Gabr, K. Thorlund, C. Balijepalli, et al., Cardiovasc. Intervent. Radiol. 40 (2017) 1033–1043. doi: 10.1007/s00270-017-1594-4
Y. Qian, Q. Liu, P. Li, et al., ACS Nano 15 (2021) 2933–2946. doi: 10.1021/acsnano.0c09122
V. Pretet, A.L. Giraudet, L. Vergnaud, et al., Clin. Nucl. Med. 49 (2024) 584–586. doi: 10.1097/rlu.0000000000005212
D. Wang, L. Zhang, W.H. Yang, et al., Adv. Sci. 12 (2025) e2410484. doi: 10.1002/advs.202410484
L. Zhang, D. Wang, L.Z. Zhang, et al., Biomaterials 316 (2025) 123018. doi: 10.1016/j.biomaterials.2024.123018
X. Liang, H. Liu, H. Chen, et al., Aggregate 5 (2024) e552. doi: 10.1002/agt2.552
L. Li, Y. Cao, H. Zhang, et al., J. Nanobiotechnol. 21 (2023) 413. doi: 10.1109/peas58692.2023.10395850
H. Li, K. Qian, H. Zhang, et al., Chem. Eng. J. 418 (2021) 129534. doi: 10.1016/j.cej.2021.129534
M.J. Mitchell, M.M. Billingsley, R.M. Haley, et al., Nat. Rev. Drug Discov. 20 (2021) 101–124. doi: 10.1038/s41573-020-0090-8
T.G. Dacoba, S. Anthiya, G. Berrecoso, et al., Adv. Funct. Mater. 31 (2021) 2009860. doi: 10.1002/adfm.202009860
T. Nakamura, K. Kawakami, M. Nomura, et al., J. Control. Release 345 (2022) 200–213.
S. Wilhelm, A.J. Tavares, Q. Dai, et al., Nat. Rev. Mater. 1 (2016) 16014. doi: 10.1038/natrevmats.2016.14
D.J. Irvine, E.L. Dane, Nat. Rev. Immunol. 20 (2020) 321–334. doi: 10.1038/s41577-019-0269-6
Z. Liu, W. Jiang, J. Nam, et al., Nano Lett. 18 (2018) 6655–6659. doi: 10.1021/acs.nanolett.8b02340
A. Amouzegar, M. Chelvanambi, J.N. Filderman, et al., Cancers 13 (2021) 2695. doi: 10.3390/cancers13112695
Q. Lu, D. Kou, S. Lou, et al., J. Hematol. Oncol. 17 (2024) 16.
Z. Zhang, H. Wang, T. Tan, et al., Adv. Func. Mater. 28 (2018) 1801840.
H. Wang, S. Sun, Y. Zhang, et al., Drug Deliv. 26 (2019) 89–97. doi: 10.1080/10717544.2018.1561766
S.N. Bhatia, X. Chen, M.A. Dobrovolskaia, et al., Nat. Rev. Cancer 22 (2022) 550–556. doi: 10.1038/s41568-022-00496-9
H. Cheng, X. Fan, E. Ye, et al., Adv. Mater. 34 (2022) 2107674.
W. Wang, Y. Jin, X. Liu, et al., Adv. Funct. Mater. 31 (2021) 2100386.
A.A. D’Souza, R. Shegokar, Expert Opin. Drug Deliv. 13 (2016) 1257–1275. doi: 10.1080/17425247.2016.1182485
C. Zhu, L. Ke, X. Ao, et al., Adv. Mater. 36 (2024) e2310078.
R. Devulapally, K. Foygel, T.V. Sekar, et al., ACS Appl. Mater. Interfaces 8 (2016) 33412–33422. doi: 10.1021/acsami.6b08153
D. Schmid, C.G. Park, C.A. Hartl, et al., Nat. Commun. 8 (2017) 1747.
Z. Yu, J. Guo, M. Hu, et al., ACS Nano 14 (2020) 4816–4828. doi: 10.1021/acsnano.0c00708
Y.P. Fan, J.Z. Liao, Y.Q. Lu, et al., Mol. Ther. Nucleic Acids 7 (2017) 181–189.
J. Chen, Y. Zhan, Y. Wang, et al., Acta Biomater. 80 (2018) 154–168.
X. Zhang, H. Zhang, L. Yin, et al., J. Biomed. Nanotechnol. 12 (2016) 1688–1698. doi: 10.1166/jbn.2016.2278
M.J.C. Espinoza, K.S. Lin, M.T. Weng, et al., Int. J. Biol. Macromol. 228 (2023) 487–497.
Z. Yang, D. Gao, J. Zhao, et al., Nat. Rev. Clin. Oncol. 20 (2023) 116–134. doi: 10.1038/s41571-022-00717-y
Q. Liu, J. Zou, Z. Chen, et al., Acta Pharm. Sin. B 13 (2023) 4391–4416.
J. Zhang, Y. Lin, Z. Lin, et al., Adv. Sci. 9 (2022) e2103444.
H. Cabral, H. Kinoh, K. Kataoka, Acc. Chem. Res. 53 (2020) 2765–2776. doi: 10.1021/acs.accounts.0c00518
Y. Shi, T. Lammers, Acc. Chem. Res. 52 (2019) 1543–1554. doi: 10.1021/acs.accounts.9b00148
M.W. Khan, P. Zhao, A. Khan, et al., Int. J. Nanomedicine 14 (2019) 3753–3771. doi: 10.2147/ijn.s196651
S. Tang, C. Fu, L. Tan, et al., Biomaterials 133 (2017) 144–153.
H. Ju, Y. Cui, Z. Chen, et al., Am. J. Transl. Res. 8 (2016) 1838–1847.
F.Q. Wu, T. Fang, L.X. Yu, et al., J. Hepatol. 65 (2016) 314–324.
X. Gao, H. Cheng, M. Teng, et al., J. Control. Release 379 (2025) 879–889.
L. Wei, D. Lee, C.T. Law, et al., Nat. Commun. 10 (2019) 4681.
D. Su, Bioengineered 12 (2021) 11124–11135. doi: 10.1080/21655979.2021.2001239
G. Lin, J. Chen, X. Liu, et al., Chin. Chem. Lett. 36 (2025) 111018. doi: 10.1016/j.cclet.2025.111018
G.F. Luo, W.H. Chen, X. Zeng, et al., Chem. Soc. Rev. 50 (2021) 945–985. doi: 10.1039/d0cs00152j
E.J. Comparetti, P.M.P. Lins, J. Quitiba, et al., J. Biomed. Mater. Res. A 110 (2022) 1499–1511. doi: 10.1002/jbm.a.37387
Y. Wang, Q. Zhao, B. Zhao, et al., Adv. Sci. 9 (2022) 2105631.
F. Wang, L. Li, K. Piontek, et al., Hepatology 67 (2018) 940–954. doi: 10.1002/hep.29586
W. Ma, D. Zhu, J. Li, et al., Theranostics 10 (2020) 1281–1295. doi: 10.7150/thno.40291
J. Guo, M. Gu, Y. Chen, et al., Chin. Chem. Lett. 36 (2025) 110849. doi: 10.1016/j.cclet.2025.110849
A.M. Gutierrez, E.M. Frazar, M.V.X. Klaus, et al., Adv. Healthc. Mater. 11 (2022) e2101820.
R.S. Riley, C.H. June, R. Langer, et al., Nat. Rev. Drug Discov. 18 (2019) 175–196. doi: 10.1038/s41573-018-0006-z
A. Singh, N.A. Peppas, Adv. Mater. 26 (2014) 6530–6541. doi: 10.1002/adma.201402105
Y. Chao, Q. Chen, Z. Liu, Adv. Func. Mater. 30 (2020) 1902785.
J.Q. Zhu, H. Wu, X. Li, et al., Adv. Sci. 11 (2023) e2305508.
L. Lei, D. Huang, H. Gao, et al., Sci. Adv. 8 (2022) eadc8738.
N. Oliva, J. Conde, K. Wang, et al., Acc. Chem. Res. 50 (2017) 669–679. doi: 10.1021/acs.accounts.6b00536
F. Cheng, T. Su, S. Zhou, et al., Sci. Adv. 9 (2023) eade6257.
F. Wang, D. Xu, H. Su, et al., Sci. Adv. 6 (2020) eaaz8985.
M. Sonker, S. Bajpai, M.A. Khan, et al., ACS Appl. Bio Mater. 4 (2021) 8080–8109. doi: 10.1021/acsabm.1c00857
N. Falcone, M. Ermis, A. Gangrade, et al., Adv. Func. Mater. 34 (2023) 2309069.
Q. Liu, R. Xu, J. Shen, et al., J. Transl. Med. 22 (2024) 341.
C. Song, H. Phuengkham, Y.S. Kim, et al., Nat. Commun. 10 (2019) 3745.
B. Farasati Far, A.A. Isfahani, E. Nasiriyan, et al., Livers 3 (2023) 161–189. doi: 10.3390/livers3020012
Y. Peng, H. Liu, X. Liang, et al., J. Control. Release 380 (2025) 1–16. doi: 10.11922/11-6035.csd.2024.0081.zh
J. Meng, X. Yang, J. Huang, et al., Adv. Sci. 10 (2023) 2300517.
Z. Meng, X. Zhou, J. Xu, et al., Adv. Mater. 31 (2019) e1900927.
X. Li, N. Gong, F. Tian, et al., Nat. Biomed. Eng. 7 (2023) 1129–1141. doi: 10.1038/s41551-023-01084-4
E. Ahnfelt, O. Degerstedt, E. Lilienberg, et al., J. Drug Deliv. Sci. Technol. 53 (2019) 101143.
A. Pérez-López, C. Martín-Sabroso, L. Gómez-Lázaro, et al., Acta Biomater. 149 (2022) 1–15.
Y.M. Nouri, J.H. Kim, H.K. Yoon, et al., Korean J. Radiol. 20 (2019) 34–49. doi: 10.3348/kjr.2018.0088
R. Lencioni, J.M. Llovet, Semin. Liver Dis. 30 (2010) 52–60.
S. Wu, K. Fan, Q. Yang, et al., J. Nanobiotechnology 21 (2023) 42.
G. Jia, J.V. Valkenburgh, A.Z. Chen, et al., Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 14 (2022) 1749. doi: 10.1007/s13369-021-06090-9
K.H. Lee, E. Liapi, J.A. Vossen, et al., J. Vasc. Interv. Radiol. 19 (2008) 1490–1496.
K. Malagari, M. Pomoni, H. Moschouris, et al., Cardiovasc. Intervent. Radiol. 37 (2014) 165–175. doi: 10.1007/s00270-013-0777-x
P. Huppert, T. Wenzel, H. Wietholtz, Cardiovasc. Intervent. Radiol. 37 (2014) 154–164. doi: 10.1007/s00270-013-0632-0
E. Dhondt, B. Lambert, L. Hermie, et al., Radiology 303 (2022) 699–710. doi: 10.1148/radiol.211806
J.F. Nijsen, A.D. van het Schip, W.E. Hennink, et al., Curr. Med. Chem. 9 (2002) 73–82. doi: 10.2174/0929867023371454
H. Petrowsky, R. Fritsch, M. Guckenberger, et al., Nat. Rev. Gastro. Hepat. 17 (2020) 755–772. doi: 10.1038/s41575-020-0314-8
J. Zhong, Q. Zhang, G. Kuang, et al., Chem. Eng. J. 455 (2023) 140585.
M. Chen, G. Shu, X. lv, et al., Biomaterials 284 (2022) 121512.
Q. Li, Y. Liu, X. Guo, et al., Biomed. Pharmacother. 151 (2022) 113123.
A. Zhang, Z. Xiao, Q. Liu, et al., Adv. Healthc. Mater. 10 (2021) 2100748.
Z. Zheng, M. Ma, X. Han, et al., Acta Biomater. 157 (2023) 337–351.
L. Liu, X. Liang, X. Xu, et al., Acta Biomater. 130 (2021) 374–384.
N. Yang, X. Sun, Y. Zhou, et al., Sci. Bull. 68 (2023) 1772–1783.
F. Deschamps, T. Isoardo, S. Denis, et al., Acta Biomater. 87 (2019) 177–186.
H. Liu, T.A. Zhang, W.Y. Zhang, et al., Exp. Neurol. 369 (2023) 114541.
X. Liao, X. Song, J. Li, et al., Acta Biomater. 149 (2022) 82–95.
J. Li, C. Wang, X. Han, et al., ACS Appl. Mater. Interfaces 14 (2022) 45167–45177. doi: 10.1021/acsami.2c12869
C. Ye, J. Zhang, J. Shen, et al., Chin. Chem. Lett. 36 (2025) 110519.
X. Xia, Y. Li, R. Huang, et al., Adv. Sci. 12 (2024) 2410873.
T. Yoshimoto, S. Imura, Y. Morine, et al., Anticancer Res. 38 (2018) 501.
Z. Peng, W. Fan, B. Zhu, et al., J. Clin. Oncol. 41 (2022) 117–127. doi: 10.1002/9783527816699.ch6
Y. Xia, W. Tang, X. Qian, et al., J. Immunother. Cancer 10 (2022) e004656. doi: 10.1136/jitc-2022-004656
S. Zuo, J. Song, J. Zhang, et al., Theranostics 11 (2021) 7471–7487. doi: 10.7150/thno.59953
D. Ho, X. Sun, S. Sun, Acc. Chem. Res. 44 (2011) 875–882. doi: 10.1021/ar200090c
S. Peng, F. Xiao, M. Chen, et al., Adv. Sci. 9 (2022) 2103836.
B. Gao, J. Luo, Y. Liu, et al., Int. J. Nanomedicine 16 (2021) 4073–4085. doi: 10.2147/ijn.s308057
Q. Wu, Z. He, X. Wang, et al., Nat. Commun. 10 (2019) 240.
S. Yang, C. Cai, H. Wang, et al., Cell Commun. Signal. 20 (2022) 26.
M. Moazzam, M. Zhang, A. Hussain, et al., Mol. Ther. 32 (2024) 284–312.
L. Li, H. Wang, Cancer Lett. 379 (2016) 191–197.
X. Liu, Z. Wu, C. Guo, et al., Drug Deliv. 29 (2022) 138–148. doi: 10.1080/10717544.2021.2021324
M. Yang, J. Li, P. Gu, et al., Bioact. Mater. 6 (2021) 1973–1987.
M. Planque, S. Igelmann, A.M. Ferreira Campos, et al., Curr. Opin. Chem. Biol. 76 (2023) 102362.

Scheme 1 Schematic diagram of micro-nanomaterials as drug delivery systems for remodeling the TIME of HCC. Created with BioRender.com.

Figure 1 The clinical transformation of micro and nanomaterials for HCC immunotherapy. In terms of materials, it is important to consider safety, large-scale production, quality control, and long-term stability. In animal experiments, it is necessary to have tumor models that more closely resemble human conditions and to adjust the dosage accordingly. In clinical treatment, achieving more accurate diagnosis, personalized treatment plans, cost-effective therapies, and favorable prognosis is crucial. Collaborative efforts from interdisciplinary scholars, along with continuous technological innovations, will provide a promising outlook for clinical translation. Created in BioRender.com.

 扫一扫看文章
扫一扫看文章

扫一扫关注我们
 DownLoad:
DownLoad:
 下载:
下载:
 下载:
下载: