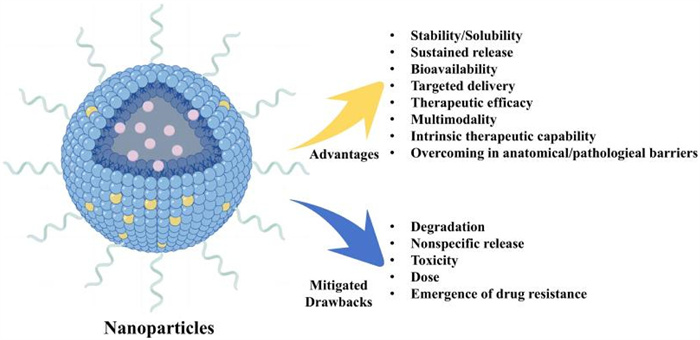
Figure 1.
The key features of colon-targeted NDDS. NDDS can be modified in various ways to surmount the hurdles associated with colon-targeted oral drug delivery.
Nanotechnology-based natural remedies: Advancing inflammatory bowel disease treatment through targeted drug delivery
Luqing Zhao , Dan Dou , Di Zhang , Shuqing Wang , Xihan Zhu , Ning Ding , Shengsheng Zhang , Chao Li

Inflammatory bowel disease (IBD) is a group of chronic conditions characterized by inflammation in the gastrointestinal tract, which includes Crohn’s disease and ulcerative colitis (UC). It is marked by symptoms such as abdominal pain, diarrhea, and bloody stools. The incidence of IBD has risen markedly in the 21st century, with an estimated 6.8 million people worldwide living with the condition in 2017—an 85% increase since 1990 [1]. The exact cause of IBD is not fully understood, but it is thought to involve a combination of genetic predisposition, immune system dysfunction, and environmental factors. The underlying pathogenesis is associated with an inappropriate immune response to the normal gut microbiota in susceptible individuals, leading to ongoing inflammation and tissue damage within the digestive tract.
Current therapeutic strategies for IBD are primarily focused on the induction and maintenance of remission, with a reliance on treatments such as 5-aminosalicylic acid (5-ASA), corticosteroids, immunosuppressants, and biological agents. These approaches have shown success in managing symptoms and improving patient quality of life [2]. However, they are not without challenges, including the potential for relapse and the long-term risks associated with adverse effects and immunosuppression. The financial burden of sustained medical treatment and the risk of treatment-related complications further emphasize the need for novel, cost-effective therapeutic solutions.
A burgeoning interest in harnessing natural compounds as an adjunct to IBD management has emerged, heralding novel complementary therapeutic avenues. Natural products, derived from plants, herbs, and other organic sources, have exhibited potent anti-inflammatory properties, hinting at their capacity to positively influence the trajectory of IBD. They boast several advantages, including cost-effectiveness, a more favorable side effect profile, and a track record of safe utilization [3]. However, their clinical deployment is frequently impeded by low bioavailability and chemical lability. There is an acute necessity to bolster the therapeutic impact of natural products in the treatment of IBD.
Advancements in nanotechnology have yielded efficacious remedies to these impediments, particularly by augmenting the bioavailability and precision targeting of natural compounds [4]. Nanoparticle (NP)-based delivery systems stand out as a promising solution, providing a mechanism to ameliorate the solubility, stability, and assimilation of natural remedies [5]. Diminishing particle size to the nanoscale escalates surface area, substantially accelerating the dissolution rate and bioavailability of hydrophobic medications [6]. Nanotechnology’s malleability further permits the crafting of carrier systems that can encapsulate and safeguard natural compounds, with nanocarriers proving pivotal in shielding these entities from premature degradation in the gastrointestinal tract and in instituting a more measured release regimen. This fine-tuned management of drug release represents a notable advancement, facilitating sustained and directed therapeutic conveyance. As research advances, the transformative potential of nanotechnology in the arena of natural medicine is progressively coming to the fore.
This review endeavors to collate the extant applications of natural product-driven NP delivery systems within the holistic treatment paradigm of IBD, while also furnishing a reference point for prospective future therapeutic modalities. The scholarly landscape has witnessed several reviews on this subject in recent years. For instance, Sun et al. delineated the pathophysiological microenvironment of IBD-inflammation sites and distilled the quintessential nano-therapeutic strategies for IBD via both passive and active targeting mechanisms inherent in nanotechnology-based nano-medicines [7]. Moreover, they cast a spotlight on the emergent prodrug-based therapeutics, encompassing 5-aminosalicylic acid, and prodrugs conjugated with amino acids and carbohydrates. Zhang et al. scrutinized the diverse administration pathways and targeting tactics for nanotherapeutics in IBD treatment, with a pronounced emphasis on nano-therapy approaches predicated on the distinct pathogenesis of IBD [8]. Li et al. deliberated on the efficacy of synthetic NPs freighted with bioactive constituents sourced from medicinal plants, such as berberine (BBR), quercetin (QT), and curcumin (CUR), in IBD management, underscoring the critical role of extracellular carriers (EVs) in transporting efficacious active chemical entities from medicinal plants to effectuate IBD treatment [9]. Zhou et al. offered a comprehensive summary of the targeting principles underpinning micro/nano delivery systems for the conveyance of natural products in IBD therapy, elucidating the synergistic interplay between targeted and responsive release strategies of these delivery systems and their anti-inflammatory efficacy within IBD animal models [10]. Yet, in juxtaposition with these existing articles, the significance and innovation of our review are twofold: it delivers a sweeping and meticulous appraisal, encapsulating the vast majority of the aforementioned articles’ pivotal content, and it provides an exhaustive emphasis on the evolution of diverse nanocarriers-encompassing polymeric NPs, metallic and inorganic NPs, and lipid-based NPs—suitable for the carriage of natural products, alongside an in-depth exploration of the mechanisms through which nanotechnology-empowered natural remedies ameliorate IBD. Consequently, this review affords readers a more profound comprehension of the research advancements and applications of natural product nano-delivery systems in the targeted therapy of IBD, as well as the foundational precepts and therapeutic dynamics of a variety of nano-delivery pharmaceuticals.
NPs have become widely acknowledged as a highly potent platform within the spectrum of drug delivery systems (DDSs) due to their inherent benefits (Fig. 1). These include their small size, which confers a large surface area to volume ratio, allowing for effective encapsulation of hydrophilic and hydrophobic drugs through adsorption or covalent cross-linking. This capability enables the formation of a high local drug concentration within the carrier [11,12]. Additionally, NPs offer a stable and protective environment for drug molecules, shielding them from degradation by enzymes in the low pH environment of the stomach during drug delivery. This feature is particularly advantageous for targeted drug delivery to the inflamed colon, potentially enhancing therapeutic efficacy and reducing the frequency of administration [13,14]. In this section, we will discuss various types of NPs, including lipid-based NPs, polymeric NPs, metallic NPs, plant-derived exosomes, and mesoporous silica NPs, all of which have been explored for their potential in IBD treatment. A summary of these NPs, with a focus on those reported for IBD targeting, including the context of biocompatibility and risk assessment, is provided in Table S1 (Supporting information).
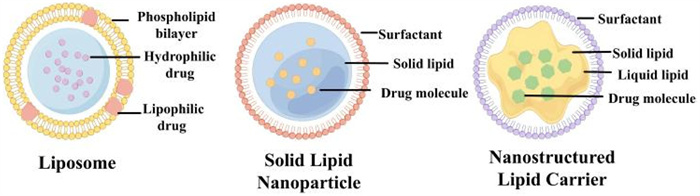
Liposomes, which encapsulate an aqueous core within a lipid bilayer, are ideal for delivering both hydrophobic and hydrophilic drugs [15]. They can significantly enhance the solubility and stability of hydrophobic components of traditional Chinese medicines (TCM) and prolong their retention time in the body [16]. Solid lipid NPs (SLNs), composed of lipids that are solid at both room and body temperatures, offer the advantage of a double-layered membrane structure, facilitating the delivery of both hydrophilic and lipophilic drugs [17,18]. Compared to liposomes, SLNs exhibit superior stability and a broader range of administration routes [19]. However, they can encounter physical instability during storage due to changes in lipid crystallinity and polymorphism [20]. To address this, Sharma et al. developed a formulation of CUR-loaded solid binary lipid NPs (SBLNs) for the oral treatment of IBD, which demonstrated reduced leucocyte infiltration, oxidative stress, and pro-inflammatory cytokine tumor necrosis factor-alpha (TNF-α) secretion, as well as maintenance of healthy colonic structure in a dextran sodium sulfate (DSS)-induced colitis model [21]. Furthermore, nanostructured lipid carriers (NLCs) were designed to overcome the limitations of SLNs, including their relatively low drug loading capacity and potential drug expulsion during storage (Fig. 2) [22]. NLCs, composed of a mixture of solid and liquid lipids, enhance the water solubility of poorly soluble substances and prolong the residence time at the target site [23]. Lertpairod et al. developed a CUR-loaded NLC formulation that provides sustained drug release at the site of colonic inflammation for up to 12 h, with the added benefit of CUR stability at room temperature for over 4 months (Fig. S1 in Supporting information) [24].
Polymer NPs are generally composed of amphiphilic polymers, which mainly consist of amphiphilic molecules with hydrophilic heads and hydrophobic tails self-assembled in aqueous solution to form a "core-shell" structure [25]. Polymer NPs can non-covalently encapsulate hydrophobic drugs in the hydrophobic core of micelles or covalently attach drugs to polymers, which can be released when stimulated by external signals, e.g., disintegration of micelles by changes in the polymer backbone configuration in IBD or induced severance of the linker arms of drug molecules on polymers [26]. Numerous polymeric NPs have been developed, with poly(lactic-co-glycolic acid) (PLGA) and chitosan (CS) predominating in particular.
PLGA is formed by the random polymerisation of two monomers, lactic acid and hydroxyacetic acid, and is a biodegradable functional polymer organic compound with many properties including simple synthesis, biodegradability, high safety, stability, and ease of modification, etc., and has been used in drug and protein/gene delivery applications due to its slow-release properties [27]. Feng et al. investigated a NP PLGA-RMP with Ramulus mori polysaccharide (RMP) encapsulated in PLGA, which promoted the expression of anti-inflammatory cytokines and the production of short-chain fatty acids (SCFAs) and attenuated the accumulation of pro-inflammatory cytokines in colitis showed a significant therapeutic effect on a mouse model of colitis [28]. Since PLGA gives the nanocarrier a good water solubility and stability, helping the nanocarrier escape the phagocytosis of the reticuloendothelial system to increase the circulation time. Zhou et al. used PLGA and PLGA-PEG-MAL loaded andrographolide (AG)/CORM-2 to form AG/CORM-2@NP and AG/CORM-2@NP-Dex (linked with dextran (Dex) via a thiolmaleimide click chemistry reaction to improve the active targeting ability) (Fig. S2 in Supporting information), for synergistically anti-inflammatory/pro-resolving treatment of UC, which down-regulated the expression of pro-inflammatory cytokines and reduced myeloperoxidase (MPO) activity in DSS induced colitis model [29].
Chitin is one of the most abundant natural amino polysaccharides obtained from the components of cell walls in fungi, certain hard structures in invertebrates and fish. CS was obtained by alkaline hydrolysis of chitin, which is a natural linear polysaccharide cationic and hydrophilic polymer [30]. Due to its simple preparation and abundant sources, it is now frequently used as a non-toxic, biocompatible, and biodegradable novel carrier for drug delivery. Positively charged amino groups (-NH3+) on the surface of CS NPs can specifically interact with negatively charged mucosal surfaces at the site of colonic inflammation to achieve prolonged drug release and enhanced colonic drug absorption. However, CS breaks down so readily at gastric acid pH that the drug is released in large quantities before it reaches the colonic site, often made with alginate or other molecules into NPs that are stable under acidic conditions for targeted release in the gut [31]. Sodium alginate (SA) was incorporated into CS NPs by Sun et al. to obtain a type of SA-CS NPs with enhanced ability to penetrate the mucus layer of the colon while loaded with the TCM berberine hydrochloride (BH) for oral treatment of UC [32]. Therapeutic effectiveness demonstrated that in DSS-induced colitis rats, BH-SA-CS NPs could not only alleviate colonic injury, but also improve the immunologic function. To avoid QT be absorbed in the stomach and small intestine, Khater et al. assembled QT and CS NPs as QT-NPs, which alleviate inflammation and oxidative stress by controlling tight junction (TJ)-related genes and redox imbalance and inflammation in DSS-induced colitis rats [33].
HN are another kind of polymeric NPs with the diameters of 1–1000 nm [34], which created by chemically or physically connected swellable polymer networks and water is their main dispersion medium [34,35]. Interestingly, different physical, chemical and biological signals can easily and precisely manipulate the formation, degradation, multiscale shape, architecture and functions of HN [36]. Of note, HN have been studied extensively and utilized for several biomedical applications, offering strengths like benign biocompatibility, active ingredient protection highly structural designability, enhanced bioavailability [37,38]. A combination of CUR-loaded carboxymethyl CS (CC) microspheres and hyaluronic acid (HA) and gelatin (GE) hydrogels (HA-GE) was designed as a composite DDS, which associated the drug protection effect of CC with the intelligent release action of HA-GE, enhances the therapeutic effect of CUR in colon site so as to improve the bioavailability of CUR [39].
Metallic NPs are a special and valuable class of promising nanomaterials for biomedical applications, which mainly refer to gold and silver NPs [40]. Gold is known for inhibiting the secondary response in terms of both the production of inflammatory and anti-inflammatory factors [41], while silver has been widely used due to its antimicrobial properties [42]. Due to their biocompatibility, controllable size, shape, and charge, as well as versatile surface modifications [43,44], metallic NPs are widely employed in several fields, ranging from diagnostic and therapeutic applications to colon-targeted DDSs [45–47]. Compared with the other NPs, metallic NPs can easily be taken up by cells according to the high density [48]. Considering the anti-inflammatory properties of CUR and the ability to suppress microbial activity and promote wound healing that silver has, Piotrowska et al. combined CUR and silver to synergistically enhance their activity. The result providing the information that with the combination of CUR and silver can not only decreased colon damage in DSS-induced mouse model of colitis via increasing the bioavailability of CUR, but also minimized the toxic effects of silver NPs [49]. A type of silver NPs derived from blackcurrant was developed, which are able to alleviated colitis by a decreased MPO activity in DSS-induced mouse model of colitis, indicating it is a reasonable way of silver NPs to be used in IBD treatment [50].
Exosomes are membrane vesicles secreted from a variety of cell types and are found in a wide range of biological fluids, including blood, urine, saliva, and amniotic fluid [51]. Exosomes have a variety of biological functions such as intercellular communication, but recent studies have found that exosomes can cross the blood-brain barrier and be used as targeted drug delivery vectors, a finding that has attracted significant attention because exosomes are less immunogenic than liposomes and viral-based DDSs [52,53]. For example, exosome-based CUR nanovesicles have been shown to improve the stability and solubility of CUR through physical embedding [54]. Zhu et al. demonstrated that Portulaca oleracea L-derived exosome-like NPs (PELNs) shows excellent stability and safety within the gastrointestinal tract of DSS-induced C57 mice while displaying a significant targeting to inflamed colon sites [55]. Moreover, Ginseng-derived exosome-like NPs (GENs) can modulate the intestinal microbiota and immune microenvironment, and are considered as an effective approach in UC therapy [56].
MSNs have high porosity and specific surface area, which can achieve high drug loading and controlled drug release [57]. They can be modified with functional molecules to form pH, temperature, redox, and enzyme-sensitive MSNs [58]. In recent years, functionalized MSNs have attracted much attention. Organofunctionalized silica formed by introducing a series of targeting components into the framework can improve drug utilization and enhance biodegradation compared to ordinary MSNs. Jiang et al. prepared an oral delivery vehicle of tetrasulphide-containing organosilica NPs (DSMSNs) encapsulated by resveratrol (Res) functionalized by the targeting component CS, loaded with Res (Fig. S3 in Supporting information). In inflammatory environments, tetrasulfide-containing (S-S-S-S) MONs break down in response to GSH specifically, which enables rapid disassembly of DSMSNs and efficient release of Res, indicating that the recovery of gut microbial diversity in the colitis model to mitigate colonic inflammation, in order to achieve therapeutic effects in UC [59].
With the development of nanotechnology in recent years, more and more response mechanisms have been explored. Due to the diversity of the structure and composition of nanomaterials and the advantages of easy functional modification, we can design stimuli-responsive nanomaterials to achieve responsive targeted release of drugs based on some special physicochemical characteristics of the lesion site [60]. Some studies have shown that the design of stimuli-responsive nanomedicine carriers based on the pathophysiological changes of IBD can effectively avoid the premature release of the drug, and greatly reduce the toxic side effects of drug leakage prematurely in the transport process [61]. Therefore, in this part we summarized the most common response mechanisms, including trigger-release (pH-responsive, reactive oxygen species (ROS)-responsive and enzyme-responsive), charge-mediated, ligand-receptor targeted as well as multi-responsive mechanisms. The characteristics of these mechanisms are shown in Table S2 (Supporting information).
Due to the varying pH values across the gastrointestinal tract, targeted mechanisms can be designed for specific regions. Under normal physiological conditions, the pH in the stomach is 1.2, the pH in the small intestine is 6.5–7.5, and the pH in the colon ranges from 6 to 8.6. In inflammatory environments, the colonic pH (2.3–5.5) of patients with IBD is lower than that of normal conditions [62]. The method of targeting the colon involves coating a pH-dependent polymer onto a carrier to protect the drug from degradation in the stomach, ensuring the delivery of the drug to a specific area of the colon. Most pH-sensitive carriers are very safe and can quickly dissolve or expand at specific pH values, promoting drug release and absorption in specific areas [63]. Jacob et al. designed the formulation of pH-sensitive biodegradable garcinol (GAR)-loaded PLGA coated with Eudragit® S100 (GAR-PLGA-ES100 NPs) by using a solvent evaporation technique [64]. In vitro drug release studies, they dissolved NPs in solutions of different pH values, simulating the stomach (pH 1.2), small intestine (pH 5.6), and large intestine (pH 7.4), respectively. The results showed that GAR from GAR-PLGA-ES100 NPs was released the most at pH 7.4 compared with pH 1.2 and 5.6 and able to withstand drug release at an acidic pH resembling the stomach and small intestine. Gugulothu et al. formulated Eudragit® S100 NPs loaded with CUR-celecoxib combination (Cur-CelNPs) [65]. This polymer dissolves at the pH 7.0 by ionization of its carboxylic functional group and thus has been used for targeting drugs to the colonic region of gastrointestinal tract. In the 2,4,6-trinitrobenzenesulfonic acid (TNBS)-induced UC rat experiment, Cur-CelNPs significantly reduced the levels of MPO and lactoperoxidase (LPO) in the colon of rats, and increased the levels of SOD. Moreover, Cur-CelNPs were found to be more effective than the suspension of the drugs, indicating the potential of pH-sensitive NPs for treating UC. Like most carriers, although these can effectively prevent drug release in the stomach and small intestine to ensure delivery to the colon, they still cannot achieve precise release of weak acid environment in the intestines of IBD patients. Zhang et al. coated two pH-sensitive materials, Eudragit® EPO and L100, on nanoscale CUR to fabricate core-shell NPs (CNs@EPO@L100) [66]. Solutions with pH 1.2, 6.8, and 3.0 were used to simulate the environment of the stomach, small intestine, and inflamed colon, respectively. Due to the dual protection of L100 slowing down the dissolution of pH 1.2 and EPO slowing down the dissolution of pH 6.8, the NPs can ultimately be released in large quantities to the inflamed colon (pH 3.0). In the DSS-induced UC mice experiment, CNs@EPO@L100 also showed good therapeutic effects (Fig. S4a in Supporting information). However, the pH of the colon in IBD patients may vary due to inherent inter individual/intra individual variations, disease status, and feeding conditions. Therefore, pH-response based solely on gastrointestinal pH is not reliable in colon targeted therapy.
ROS are a class of oxygen-derived chemicals produced by the human body, which play an important role in the pathological and physiological processes of various gastrointestinal diseases, including IBD. Under normal physiological conditions, there is a steady-state balance between the production of ROS and the removal of endogenous antioxidant scavenging compounds. The intestinal mucosa of IBD patients is characterized by severe disorders of antioxidants and the overproduction of ROS, leading to oxidative stress and mucosal injury [67]. Overproduction of ROS is also a direct causative agent for dysregulated signal transduction, inflammatory response and DNA damage. By utilizing the pathological conditions of IBD, the ROS-responsive mechanism has become an area of interest in improving targeted drug delivery strategies in the inflammatory intestinal region. Zhao et al. covalently linked modified BBR derivatives with o-diphenol structure via aryl borate esters as a responsive connector to CC to form OC-B-BBR nano micelles. The borate bond was broken under excess ROS conditions to release BBR molecules, thereby enabling effective delivery of the encapsulated BBR to the site of inflammation. In an experiment of DSS-induced mice, the effective release of drugs under oxidative stress microenvironment promotes the downregulation of interleukin-6 (IL-6) expression levels in the system, reshapes the gut microbiota, and significantly alleviates symptoms of colitis and colon injury [68]. Luteolin (LUT) is a natural antioxidant with effective free radical scavenging and cell protective properties [69]. Unfortunately, like most flavonoids, LUT is easily oxidized and degraded due to its highly unsaturated structure, and is limited by its poor water solubility, low bioavailability, and short half-life. Tan et al. developed ROS-responsive NPs as an efficacious nanomedicine against UC with oral administration. The NPs were fabricated with a D-α-tocopherol polyethylene glycol succinate-b-poly(β-thioester) copolymer (TPGS-PBTE) for ROS cleavage via the colitis-targeted delivery of LUT. Due to the oxidation of the thioether bond in the main chain of the copolymer by reactive oxygen species, it induces a hydrophilic-to-hydrophobic transition, leading to the hydrolysis and release of LUT [70]. With the help of the delivery system, LUT is effectively delivered and released in the ROS-rich colonic regions through carrier degradation. In a DSS-induced acute colitis murine model, LUT@TPGS-PBTE NPs alleviated body weight loss, colon length shortening, and damage to the colonic tissues due to the suppression of ROS and pro-inflammatory cytokines such as IL-17A, IL-6, interferon-gamma (IFN-γ) and TNF-α, as well as upregulation of anti-inflammatory factors including IL-10 and IL-4. More importantly, LUT@TPGS-PBTE NPs regulated the inflammatory microenvironment by modulating the T helper cell type 1/T helper cell type 2 (Th1/Th2) and T helper cell type 17/regulatory T cell (Th17/Treg) balance, thus resolving inflammation and accelerating the healing of the intestinal mucosa (Fig. S4b in Supporting information). However, the clinical application of ROS-responsive systems should consider some obstacles, such as cytotoxicity, stability, and biocompatibility issues.
Enzymes play a crucial role in life activities. Therefore, enzymes are selective targets for drug development and treatment. During the pathogenesis of IBD, the intestinal flora in the colon can secrete several carbohydrate-active and reductive metabolic enzymes such as β-glucosidase, cellulase, nitrogenase reductase and nitroreductase [71]. Therefore, most researchers use these enzymes as activation triggers for the release of smart DDSs at the site of lesion area. In addition, some polymer materials, such as CS, cyclodextrin (CD), and pectin, can resist enzymatic degradation in the upper digestive tract, which are degraded by these specific enzymes. Li et al. successfully prepared core-shell NPs using enteric enzymes as triggers in the controlled-release system by selecting β-CD as a carrier for CUR. CD can open the ring in response to microbial fermentation and enzymatic degradation of the colon, followed by hydrolysis of the ester bond, and the drug is released in the colon to promote colonic epithelial barrier integrity and modulate inflammatory cytokine production, remodelling the gut microbiota in DSS-induced colitis mice (Fig. S4c in Supporting information) [72]. Castangia et al. investigated the enzyme-sensitive complex of CS/nutriose polymer. QT-loaded polyethylene glycol vesicles were coated with CS and the nutriose was added to the CS [73]. The CS-nutriose complex was susceptible to enzymatic degradation in the colon and could release the QT. In the in vivo experiment of TNBS-induced colitis in mice, this complex can significantly reduce MPO and exert local anti-inflammatory effects. However, it is crucial to evaluate whether NPs can successfully and specifically release drugs in complex colon environments and variable enzymes between individuals. In addition, under disease conditions, the gastrointestinal transport time is relatively short, and the ability of enzymes to fully catalyze reactions is also a challenge.
In the affected area of the intestine of IBD patients, the mucosal components of colon mucins contain negatively charged carbohydrate. Therefore, the charged surface of inflammatory tissue can be specifically targeted by NPs with opposite charges through electrostatic interactions (i.e., cationic NPs). Studies have shown that encapsulating model proteins in bioadhesive N,N,N-trimethylchitosan chloride (TMC) NPs results in a positively charged particle surface due to protonated methyl groups, thus exhibiting good targeting ability towards negative mucins in the intestinal mucosa [74].
Oppositely, some positively charged proteins are also synthesized in large quantities in the affected colon of IBD, such as transferrin and eosinophil cationic protein [75]. Jubeh et al. studied the adhesion properties of charged liposomes to the healthy and inflamed rat intestinal epithelium [76]. The results have shown that negatively charged NPs can preferentially adhere to these cationic proteins in a rat colitis model, with negatively charged liposomes accumulate more in the inflammatory region than the cationic liposomal NPs.
In summary, studies have shown that NPs with different charges provide a method of good interaction with the affected colon and target drug delivery to the affected colon through electrostatic interactions. However, unnecessary electrostatic interactions remain problematic between these systems. For example, charged NPs may interact with negatively charged gastrointestinal components such as soluble mucins and bile acids [61].
During the pathogenesis of IBD, many specific antigens and receptors are overexpressed by intestinal epithelial cells (IEC) and activated macrophages, such as CD44, mannose receptor (MR), folate receptor (FR) and transferrin receptor (TfR). In general, targeting the diseased site through ligand-receptors can promote the accumulation of drugs and reduce drug depletion in normal tissues. Therefore, this targeting strategy can not only improve the therapeutic effect, but also reduce the occurrence of adverse events [13]. Therefore, ligand-mediated DDSs have been widely used in IBD therapy. Ye et al. prepared a sea salt polysaccharide laminarin (LA)-coated, folic acid (FA)-modified lactoferrin (LF)-NPs (LA/FA/CUR-NPs) for the delivery of the anti-inflammatory drug CUR. FA binds specifically to FA receptors (FR), and LF, a glycoprotein transferrin that binds mammalian cationic iron, can bind to LF receptors (LFR). Sea salt polysaccharide LA can effectively resist the destruction of NPs by the extreme acidic pH gastric environment, thus ensuring that it can precisely target macrophages with folate receptors and epithelial cells with transferrin receptors to alleviate inflammation, accelerate the repair of the colonic mucosal barrier and restore the balance of the intestinal flora to alleviate the symptoms of colitis (Fig. S4d in Supporting information) [77]. Konjac glucomannan (KGM) is not digested by digestive enzymes in the human upper gastrointestinal tract but can be specifically degraded by colonic β-mannanase present in the colon [78]. Wang et al. found that KGM with an acetylated structure can specifically bind to MRs that are abundantly expressed on macrophages, and thus encapsulated CUR in acetylated KGM (AceKGM) NPs to prepare a cell-containing NP that can adhere to inflammatory macrophages to Cur-AceKGM NPs, which effectively prolonged the release of CUR in the colon and improved the bioavailability of CUR [79]. The ligand-receptor-targeted mechanism shows great potential, and more natural products are waiting to be applied to treat IBD.
Currently, more and more response mechanisms are being thoroughly studied. However, it seems that each mechanism has some limitations, which cannot be separated from instability. Therefore, in order to reduce such problems, some multi responsive mechanisms have been developed to improve the treatment of IBD such as pH/ROS, pH/charge/enzyme sensitive NPs. Naeem et al. used coumarin-6 (C-6) as the model drug and prepared new NPs using a polymer mixture of enzyme-sensitive azo polyurethane and pH sensitive ES100-azo-polyurethane (ES-Azo.pu), which can ensure that particles are not released in the stomach and small intestine and azoreductase in IBD colon undergoes enzymatic reaction with azo groups in NPs, causing surface looseness and particle release (Fig. S4e in Supporting information) [80]. In vivo localization study in the rat gastrointestinal tract demonstrated that ES-Azo.pu NPs were selectively distributed in the inflamed colon, showing 5.5-fold higher C-6 than ES NPs. Li et al. developed a hierarchical structured vehicle (AP@PSi-HA@HPMCAS) based on HA functionalized PSi NPs (PSi-HA), ascorbyl palmitate (AP) and hydroxypropyl methylcellulose acetate succinate (HPMCAS) [81]. pH-responsive HPMCAS matrix will prevent premature drug release from AP@PSi-HA NPs in the GI tract until they reach or are close to the inflamed sites of intestine. After the dissolution of HPMCAS, negatively charged AP@PSi-HA NPs will then selectively bind to the inflamed sites of intestine by electrostatic adhesion, and then gradually release drug in response to inflammation due to the enzyme-labile bonds of AP. In summary, multi responsive mechanisms have better performance compared with single response mechanisms. Nevertheless, more stable and sensitive response mechanisms are waiting to be developed, and a large number of clinical trials are needed to prove their efficacy.
The pathogenesis of IBD is multifactorial, involving genetic susceptibility, immune dysregulation, and environmental factors. A key player in this complex interplay is the gut microbiota, which, when disrupted, can lead to an overactive immune response and subsequent inflammation. In this section, we explore the various mechanisms through which natural product-based nanomedicines address IBD, including immune response suppression, intestinal mucosal barrier protection, and gut microbiota regulation. We elucidate how these targeted approaches leverage the unique properties of natural products to confer their benefits and achieve therapeutic outcomes. Table S3 (Supporting information) consolidates studies on the use of such nanocarriers for IBD treatment by suppressing immune response, repairing intestinal barriers, and regulating gut microbes.
IBD is widely acknowledged to arise from abnormal immune reaction to microorganisms, particularly in those with a genetic predisposition. The chronic inflammation observed in IBD is closely linked to an overactive and imbalanced immune system. Current clinical treatments for IBD are primarily designed to suppress these immune responses. The immune response involves various components, including both innate (dendritic cells, macrophages, neutrophils, natural killer cells) and adaptive (T and B cells) immune cells, as well as the cytokines they secrete, which are instrumental in driving inflammatory pathways [82,83]. An imbalance in the immune response, due to disruptions in either innate or adaptive immunity, results in intestinal inflammation. This deregulated immune response leads to an imbalance in the production of pro- and anti-inflammatory cytokines, which cause further damage to TJ function, epithelial cell survival, and potentially the gut microbiota balance. Research has demonstrated that natural products encapsulated in NPs can navigate the biological and physicochemical barriers of the gastrointestinal tract, such as varying pH levels and enzymatic activity, to modulate immune cell recruitment and exert anti-inflammatory effects [84]. Moreover, these nanomedicines can regulate immune responses by controlling the levels of pro- and anti-inflammatory cytokines and by modulating signaling pathways.
Regulation of immune cell recruitment is a critical aspect of immune response activation. Macrophages, in particular, have a dual role in intestinal homeostasis and can polarize into either a pro-inflammatory M1 subtype or an anti-inflammatory M2 subtype [85]. M1 macrophages exacerbate intestinal injury by producing inflammatory cytokines, while M2 macrophages release anti-inflammatory cytokines to suppress immune responses. The infiltration of neutrophils is also indicative of IBD severity [86]. Natural products, such as those found in ginger, have shown promise in modulating these processes. For instance, Zhang et al. designed a pH-sensitive HA/GE composite hydrogel (CUR@gels) oral DDS containing CC microspheres loaded with CUR, which has been shown to reduce neutrophil infiltration and macrophage infiltration, thereby suppressing immune cell recruitment in colitis [39].
Supramolecular NPs, like those loading natural products, have demonstrated stability and targeting efficacy to macrophages, regulating pro- and anti-inflammatory factors and promoting M2 macrophage polarization. Han et al. devised a "supramolecular CUR NPs with pH/ROS sensitive and multistage therapeutic effects" in "advanced yeast particles" (D-mannose (Man)-CUR NYPs) delivery system, which not only showed strong stability in the complex gastrointestinal environment, but also demonstrated excellent targeting ability to macrophages (Fig. S5a in Supporting information) [87].
Similarly, Zhang et al. developed a CS-modified PLGA copolymer NP (CS-PLGA NP) system for co-delivery of patchouli alcohol (PA) and simvastatin (SV) to inflamed colonic epithelial cells to alleviate the symptoms of ulcerative colitis by remodeling the immune microenvironment, inhibiting fibroblast activation by repolarizing M2, and reducing neutrophil infiltration (Fig. S5b in Supporting information) [88]. Modulating the expression of inflammatory cytokines and signal transduction pathways is another therapeutic approach to target IBD. QT, a flavonoid found in various foods, has been encapsulated in silk fibroin NPs to enhance its stability and bioavailability, effectively reducing pro-inflammatory cytokine expression (TNF-α, IL-1β, and IL-6) [89]. Local drug administration can maximize treatment efficacy, and enemas show promise in this regard. Rutin, another flavonoid, when contained in a hydrogel system for targeted delivery by enema administration, significantly inhibited overexpressed inflammatory cytokines TNF-α and IL-6 in a mouse model of colitis, showing improved therapeutic efficacy (Fig. S5c in Supporting information) [90].
Nanocarriers loaded with natural products have been widely recognized as novel DDSs. The current research shows that nanomaterials not only play the role of delivering drugs to target inflammatory sites, but also have anti-inflammatory effects and the function of regulating the immune microenvironment [91]. For the therapeutic drugs for IBD that have been used in clinical practice, nanomaterials can prolong the circulation period and reduce the side effects of clinical drugs by improving drug encapsulation efficiency and targeted drug delivery. The application of nanotechnology improves the hydrophobic properties of some natural products with anti-inflammatory components, which exert anti-inflammatory effects by affecting inflammatory pathways and regulating inflammatory cells or inflammatory factors.
The intestinal barrier, comprised of a monolayer of epithelial cells and various other cell types, plays a crucial role in innate immunity [92,93]. TJs are integral to this barrier, maintaining the selective permeability of the gut and preventing the passage of harmful substances. Disruption of the intestinal barrier is intricately connected to the development of IBD, with the loss of TJ proteins leading to leakage and subsequent immune system activation. Restoration of the epithelial barrier is thus a significant therapeutic goal for IBD treatment [94,95].
To date, nanomedicines have been developed to enhance drug delivery to the intestinal epithelium and overcome the biological and physicochemical barriers of the gastrointestinal tract. Rhein (RH), a natural anthraquinone compound, has been shown to modulate inflammatory pathways and repair intestinal barrier damage by upregulating TJ proteins. The use of pH/ROS-sensitive polysaccharide-based NPs loaded with RH has demonstrated significant repair of the colonic mucosal barrier by up-regulating the expression of TJ proteins including ZO-1, claudin-1 and occludin in vivo, as depicted in Fig. S5d (Supporting information) [96].
To specifically target diseased colonic tissue, active targeting strategies against colonic epithelial cells have been explored. LA-coated, FA-modified LF NPs were used to encapsulate CUR (LA/FA/CUR-NPs) with a food grade, enzyme-sensitive, and dual-targeting capability. LA/FA/CUR-NPs were able to specifically target colonic epithelial cells and macrophages via LF and FA ligands, respectively, to enhance uptake efficiency. In DSS-induced colitis mouse model, orally administered LA/FA/CUR-NPs regulate the expression of TJ proteins (ZO-1, occludin, and claudin-1) and enhance the repairing effect of CUR on intestinal injury by targeting colonic epithelial cells in a UC mouse model [77].
Shikonin (SK) is an active ingredient extracted from the traditional Chinese herb "Zicao" (Lithospermum erythrorhizon), which is known to inhibit inflammation, regulate immunity, and promote wound healing [97]. Feng et al. used HA, CS, and pH-responsive polymer ES100 to design SK-loaded ES100/HA/CS NPs (SK@SAC), which has pH-sensitive, CD44 receptor-targeting properties that allow access to CD44 receptor-mediated macrophages, protects the intestinal barrier by enhancing the expression of intestinal epithelial TJ proteins ZO-1 and occludin In TNBS-induced IBD mice (Fig. S5e in Supporting information) [98]. As the dominant herbal drink consumed worldwide, black tea exhibits various health promoting benefits including amelioration of IBD. Several studies have found that black tea and its derivatives, such as tea polyphenols, polysaccharides, and prebiotics, significantly increase expression of TJ proteins to alleviate colitis in mice [99]. The rich content of amphiphilic molecules in tea infusion facilitates the self-assembly of colloidal particles. It was found that black tea NPs formed by the self-assembly of the main components of black tea have the effect of restoring colon epithelial cell connectivity, inhibit mucosal inflammation, and mitigate UC [100].
Generally speaking, these studies show that nano-drugs loaded with natural products can play an important role in the treatment of IBD by repairing the intestinal barrier, which not only provides a new perspective for the treatment of IBD, but also reveals the great potential of natural products in the nano-DDS (NDDS).
The gut microbiota forms an additional barrier in the mucus layer and is integral to the innate immune system’s maturation and function [101]. SCFAs produced by the microbiota have anti-inflammatory properties. Dysregulation of the gut microbiota can lead to decreased SCFA levels, increased mucosal permeability, and immune system stimulation [102,103]. The gut microbiota’s role in intestinal homeostasis is increasingly recognized, and nanocarriers loaded with natural products are seen as beneficial in regulating the gut microbiota in IBD.
As probiotic stimulator, prebiotics can promote the reproduction of probiotics and improve the functions of intestinal flora. By integrating nanotechnology, prebiotics offer a promising avenue for targeted intervention at inflammatory sites with anti-inflammatory, antiviral, and antibiotic-sparing benefits [104]. For example, an oral drug containing a prebiotically active Phellinus igniarius polysaccharide (PIP), and CS-modified PLGA nanodrug (CS-PIPP) that increased the content of SCFAs and positively regulated intestinal flora (Fig. S5f in Supporting information) [105]. RMP, another prebiotic, has been shown to have similar therapeutic effects when encapsulated in PLGA NPs. TCM, such as BBR, is a commonly utilized isoquinoline alkaloid for its anti-diarrhoeal properties [28]. Zhao et al. developed nanomicelles containing CC that encapsulated berberine (OC-B-BBR). OC-B-BBR significantly inhibited colitis by improving intestinal microbial dysbiosis. It also enhanced carbohydrate digestion and absorption, sugar metabolism, gluconeogenesis, and amino acid metabolism by increasing the abundance of beneficial bacteria and reducing the abundance of harmful bacteria (Fig. S5g in Supporting information) [68].
The gut microbiome’s metabolic state and its impact on the host at various levels are areas that require further understanding. In the fields of other diseases, nanodrugs developed targeting metabolic mechanisms have received extensive attention [106]. Modulating the gut microbiota with nano-drugs loaded with natural products offers a modern therapeutic approach for IBD and other inflammatory diseases, with the potential for the microbiome to be a key target in future IBD therapies.
In recent years, the rapidly expanding realm of nanotechnology has unveiled innovative horizons within the therapeutic domain of IBD. Therapies utilizing nanotechnology, tailored to the varied pathogenesis of IBD, have piqued interest due to their significant potential across a spectrum of IBD applications. The NPs sourced from botanical elements such as roots, stems, and leaves have notably increased in contemporary medical practices, notably within biopharmaceuticals. Capitalizing on the distinctive attributes of NPs, these platforms have illustrated their capacity to augment the bioavailability, stability, and precision targeting of natural compounds. This enhancement not only amplifies therapeutic potency but also mitigates systemic adverse effects. Moreover, an accumulating body of evidence suggests that nanomedicines derived from natural products are adept at alleviating intestinal inflammation. They achieve this by modulating immune responses, restoring the integrity of the colonic mucosal barrier, and rebalancing the intestinal microbiota.
Despite the substantial advancements in this sector, a number of scientific hurdles and pivotal technical concerns persist, posing potential impediments to the broader adoption and tangible clinical deployment of IBD nanomedicines. Prospectively, the trajectory towards clinical realization of these nanotherapies is interspersed with opportunities and challenges. The innovation of multifunctional NPs, capable of responding to diverse stimuli within the IBD microenvironment, presents an enthralling frontier. Such intelligent systems could facilitate a more bespoke and accurate therapeutic strategy. They are designed to deliver their therapeutic cargo exclusively at the inflammatory focus, thereby reducing collateral impact on healthy tissues [107].
Nevertheless, the transition from laboratory discovery to clinical application is replete with regulatory and safety considerations. The heterogeneity of nanomaterial components and their propensity for accumulation in off-target tissues may engender unpredictable or deleterious biological consequences. These may range from immunostimulatory or immunosuppressive effects to adverse side effects such as inflammation or even toxicity. Consequently, a rigorous regimen of preclinical and clinical trials is indispensable for a successful clinical transition, aiming to affirm the safety profile of these innovative therapeutic entities.
Additionally, refining the manufacturing processes to guarantee scalability, reproducibility, and economic viability represents a pivotal phase in the translational journey. Crafting robust production methodologies that can withstand the rigorous regulatory standards for pharmaceuticals is an intricate endeavor. Equally significant is an appraisal of the economic ramifications of these treatments, given the considerable financial strain they may impose on patients and healthcare infrastructure.
To encapsulate, the potential of nanotechnology in revolutionizing IBD treatment is self-evident. However, the route to clinical utilization is convoluted and necessitates a synergistic effort from diverse scientific and medical disciplines. As our comprehension of the complexities surrounding IBD etiology and NP biology deepens, the vista for transformative therapies emerges—a prospect that promises to markedly elevate the living standards for those afflicted by this debilitating ailment. The amalgamation of nanotechnology with natural therapeutics epitomizes a complementary strategy that could potentially reconfigure the benchmarks of IBD management. This holds the promise of an era where efficacious, secure, and cost-effective treatments become an accessible reality.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Luqing Zhao: Writing – original draft, Methodology, Formal analysis, Conceptualization. Dan Dou: Writing – original draft, Supervision. Di Zhang: Formal analysis, Data curation. Shuqing Wang: Formal analysis, Data curation. Xihan Zhu: Formal analysis, Data curation. Ning Ding: Data curation. Shengsheng Zhang: Writing – review & editing, Supervision, Project administration. Chao Li: Writing – review & editing, Supervision, Project administration.
Authors are thankful to the National Natural Science Foundation of China (Nos. 82341235, 82474414), Beijing Municipal Science and Technology Plan Project (No. Z221100007422094), Outstanding Young Talents Program of Capital Medical University (No. B2308), and National Leading Talents Program in Traditional Chinese Medicine (No. 2021, to Shengsheng Zhang).
Supplementary material associated with this article can be found, in the online version, at doi:
GBD 2017 Inflammatory Bowel Disease Collaborators, Lancet Gastroenterol. Hepatol. 5 (2020) 17–30. doi: 10.1016/S2468-1253(19)30333-4
C. Le Berre, S. Honap, L. Peyrin-Biroulet, Lancet 402 (2023) 571–584. doi: 10.1016/S0140-6736(23)00966-2
D.J. Newman, Natl. Sci. Rev. 9 (2022) nwac206. doi: 10.1093/nsr/nwac206
Z. Wen, L. Kang, H. Fu, et al., Carbohydr. Polym. 314 (2023) 120887. doi: 10.1016/j.carbpol.2023.120887
L. Yin, X. Jiang, M. Wang, et al., Chin. Chem. Lett. 36 (2025) 110224. doi: 10.1016/j.cclet.2024.110224
E.P. Stater, A.Y. Sonay, C. Hart, et al., Nat. Nanotechnol. 16 (2021) 1180–1194. doi: 10.1038/s41565-021-01017-9
M. Sun, W. Ban, H. Ling, et al., Chin. Chem. Lett. 33 (2022) 4449–4460. doi: 10.1016/j.cclet.2022.03.061
Y. Zhang, T. Wang, M. Sun, et al., Adv. Healthc. Mater. 12 (2023) e2300069. doi: 10.1002/adhm.202300069
N. Li, M. Wang, Z. Lyu, et al., Front. Pharmacol. 14 (2023) 1158945. doi: 10.3389/fphar.2023.1158945
Y. Zhou, X. Feng, H. Xu, et al., J. Mat. Chem. B 11 (2023) 244–260. doi: 10.1039/d2tb01965e
C.J. Wang, M.J. Byun, S.N. Kim, et al., J. Control. Release 345 (2022) 1–19.
H. Hadji, K. Bouchemal, Adv. Drug Deliv. Rev. 181 (2022) 114101. doi: 10.1016/j.addr.2021.114101
T. Zhang, G. Zhu, B. Lu, et al., Pharm. Nanotechnol. 5 (2017) 83–94. doi: 10.1117/12.2285907
X. Zhang, Y. Ma, L. Ma, et al., Carbohydr. Polym. 223 (2019) 115126. doi: 10.1016/j.carbpol.2019.115126
P.S. Zangabad, S. Mirkiani, S. Shahsavari, et al., Nanotechnol. Rev. 7 (2018) 95–122. doi: 10.1515/ntrev-2017-0154
E. Arab-Tehrany, K. Elkhoury, G. Francius, et al., Int. J. Mol. Sci. 21 (2020) 7276. doi: 10.3390/ijms21197276
S. Das, A. Chaudhury, AAPS PharmSciTech 12 (2011) 62–76. doi: 10.1208/s12249-010-9563-0
S. Pandey, F. Shaikh, A. Gupta, et al., Adv. Pharm. Bull. 12 (2022) 17–33.
R. Paliwal, S.R. Paliwal, R. Kenwat, et al., Expert Opin. Ther. Patents 30 (2020) 179–194. doi: 10.1080/13543776.2020.1720649
M. Sharma, N. Gupta, S. Gupta, RSC Adv. 6 (2016) 76621–76631. doi: 10.1039/C6RA12841F
M. Sharma, S. Sharma, J. Wadhwa, Artif. Cell. Nanomed. Biotechnol. 47 (2019) 45–55. doi: 10.1080/21691401.2018.1543191
S. Seyyedi-Mansour, M. Carpena, P. Barciela, et al., Adv. Colloid. Interface Sci. 340 (2025) 103457. doi: 10.1016/j.cis.2025.103457
N. Poonia, R. Kharb, V. Lather, et al., Future Sci. OA 2 (2016) FSO135. doi: 10.4155/fsoa-2016-0030
J. Lertpairod, W. Tiyaboonchai, J. Pharm. Investig. 52 (2022) 387–396. doi: 10.1007/s40005-022-00572-0
E.M. Pridgen, F. Alexis, O.C. Farokhzad, Expert Opin. Drug Deliv. 12 (2015) 1459–1473. doi: 10.1517/17425247.2015.1018175
M. Zu, Y. Ma, B. Cannup, et al., Adv. Drug Deliv. Rev. 176 (2021) 113887. doi: 10.1016/j.addr.2021.113887
J.A. Lee, B.G. Jung, T.H. Kim, et al., Vet. Immunol. Immunopathol. 161 (2014) 193–204. doi: 10.15870/jsers.2014.12.53.4.193
Z. Feng, S. Peng, Z. Wu, et al., Int. J. Biol. Macromol. 182 (2021) 2024–2036. doi: 10.1016/j.ijbiomac.2021.05.200
Y. Zhou, M. Yang, X. Yan, et al., ACS Appl. Mater. Interfaces 15 (2023) 36061–36075. doi: 10.1021/acsami.3c09342
B.R. Rizeq, N.N. Younes, K. Rasool, et al., Int. J. Mol. Sci. 20 (2019) 5776. doi: 10.3390/ijms20225776
S. Nalinbenjapun, C. Ovatlarnporn, J. Drug Deliv. Sci. Technol. 57 (2020) 101397. doi: 10.1016/j.jddst.2019.101397
L. Sun, X. Nie, W. Lu, et al., AAPS PharmSciTech 23 (2022) 179. doi: 10.1097/dad.0000000000002077
S.I. Khater, M.M. Lotfy, M.N. Alandiyjany, et al., Biomedicines 10 (2022) 1654. doi: 10.3390/biomedicines10071654
S.A. Ozkan, A. Dedeoglu, B.N. Karadas, et al., Turk. J. Pharm. Sci. 16 (2019) 481–492. doi: 10.4274/tjps.galenos.2019.48751
R.Z. Tang, Z.Z. Liu, S.S. Gu, et al., J. Mat. Chem. B 9 (2021) 1521–1535. doi: 10.1039/d0tb02737e
Z. Li, G. Li, J. Xu, et al., Adv. Mater. 34 (2022) e2109178. doi: 10.1002/adma.202109178
C. Li, S.R. Obireddy, W.F. Lai, Drug Deliv. 28 (2021) 1594–1602. doi: 10.1080/10717544.2021.1955042
N. Yuniarsih, A.Y. Chaerunisaa, K.M. Elamin, et al., Int. J. Nanomed. 19 (2024) 2733–2754. doi: 10.2147/ijn.s442123
S. Zhang, L. Kang, S. Hu, et al., Int. J. Biol. Macromol. 167 (2021) 1598–1612. doi: 10.1016/j.ijbiomac.2020.11.117
F. Wang, H. Yao, X. Wu, et al., Chin. Chem. Lett. 35 (2024) 108821. doi: 10.1016/j.cclet.2023.108821
B.J. Swartzwelter, F. Barbero, A. Verde, et al., Cells 9 (2020) 284. doi: 10.3390/cells9020284
S. Tang, J. Zheng, Adv. Healthc. Mater. 7 (2018) e1701503. doi: 10.1002/adhm.201701503
K. Niikura, T. Matsunaga, T. Suzuki, et al., ACS Nano 7 (2013) 3926–3938. doi: 10.1021/nn3057005
R.A. Sperling, W.J. Parak, Philos. Trans. R. Soc. A: Math. Phys. Eng. Sci. 368 (2010) 1333–1383. doi: 10.1098/rsta.2009.0273
D.R. Sakthi, A. Girigoswami, M. Siddharth, et al., Appl. Biochem. Biotechnol. 194 (2022) 4187–4219. doi: 10.1007/s12010-022-03963-z
A.K. Rengan, A.B. Bukhari, A. Pradhan, et al., Nano Lett. 15 (2015) 842–848. doi: 10.1021/nl5045378
R.M. Hussein, H. Saleh, Nanomedicine 13 (2018) 1657–1679. doi: 10.2217/nnm-2018-0009
S.N. Barnaby, A. Lee, C.A. Mirkin, Proc. Natl. Acad. Sci. U. S. A. 111 (2014) 9739–9744. doi: 10.1073/pnas.1409431111
M. Piotrowska, J.B. Krajewska, M. Talar, et al., J. Drug Deliv. Sci. Technol. 86 (2023) 104273.
J.B. Krajewska, O. Dlugosz, M. Salaga, et al., Int. J. Pharm. 585 (2020) 119549. doi: 10.1016/j.ijpharm.2020.119549
J. Mondal, S. Pillarisetti, V. Junnuthula, et al., J. Control. Release 353 (2023) 1127–1149.
M.N. Huda, M. Nafiujjaman, I.G. Deaguero, et al., ACS Biomater. Sci. Eng. 7 (2021) 2106–2149. doi: 10.1021/acsbiomaterials.1c00217
J. Li, T. Luo, D. Wang, et al., J. Adv. Res. 68 (2025) 63–74.
C. Gao, Y. Zhou, Z. Chen, et al., Theranostics 12 (2022) 5596–5614. doi: 10.7150/thno.73650
M.Z. Zhu, H.M. Xu, Y.J. Liang, et al., J. Nanobiotechnology 21 (2023) 309. doi: 10.1186/s12951-023-02065-0
J. Kim, S. Zhang, Y. Zhu, et al., J. Ginseng Res. 47 (2023) 627–637. doi: 10.1016/j.jgr.2023.01.004
H. Shirazi, M. Daneshpour, S. Kashanian, et al., Beilstein J. Nanotechnol. 6 (2015) 1677–1689. doi: 10.3762/bjnano.6.170
Z. Li, Y. Zhang, N. Feng, Expert Opin. Drug Deliv. 16 (2019) 219–237. doi: 10.1080/17425247.2019.1575806
D. Jiang, X. Xia, Z. He, et al., J. Ind. Eng. Chem. 123 (2023) 382–395. doi: 10.1016/j.jiec.2023.03.055
H. Wang, Y. Zhou, Q. Sun, et al., Front. Bioeng. Biotechnol. 9 (2021) 630352.
F. Chen, Q. Liu, Y. Xiong, et al., Int. J. Nanomed. 16 (2021) 4225–4237. doi: 10.2147/ijn.s310952
C. Yang, D. Merlin, Int. J. Nanomed. 14 (2019) 8875–8889. doi: 10.2147/ijn.s210315
C. Lautenschlager, C. Schmidt, D. Fischer, et al., Adv. Drug Deliv. Rev. 71 (2014) 58–76.
E.M. Jacob, A. Borah, S.C. Pillai, et al., Polymers 13 (2021) 862. doi: 10.3390/polym13060862
D. Gugulothu, A. Kulkarni, V. Patravale, et al., J. Pharm. Sci. 103 (2014) 687–696. doi: 10.1002/jps.23828
G. Zhang, W. Han, P. Zhao, et al., Nanoscale 15 (2023) 1937–1946. doi: 10.1039/d2nr04968f
F.A. Moura, K.Q. de Andrade, S.J. Dos, et al., Redox Biol. 6 (2015) 617–639.
L. Zhao, X. Du, J. Tian, et al., Front. Pharmacol. 12 (2021) 644387.
B.N. Rooban, V. Sasikala, D.V. Gayathri, et al., Chem. Biol. Interact. 196 (2012) 30–38.
C. Tan, H. Fan, J. Ding, et al., Mater. Today Bio 14 (2022) 100246.
X. Peng, S.E. Wilken, T.S. Lankiewicz, et al., Nat. Microbiol. 6 (2021) 499–511. doi: 10.1038/s41564-020-00861-0
S. Li, M. Jin, Y. Wu, et al., Drug Deliv. 28 (2021) 1120–1131. doi: 10.1080/10717544.2021.1934189
I. Castangia, A. Nacher, C. Caddeo, et al., Acta Biomater. 13 (2015) 216–227.
R. Coco, L. Plapied, V. Pourcelle, et al., Int. J. Pharm. 440 (2013) 3–12.
X. Zhang, Z. Yuan, J. Wu, et al., ACS Nano 17 (2023) 21116–21133. doi: 10.1021/acsnano.3c04819
T.T. Jubeh, Y. Barenholz, A. Rubinstein, Pharm. Res. 21 (2004) 447–453.
N. Ye, P. Zhao, S. Ayue, et al., Int. J. Biol. Macromol. 232 (2023) 123229.
Z. Huang, J. Gan, L. Jia, et al., Biomaterials 48 (2015) 26–36.
C. Wang, Z. Guo, J. Liang, et al., Front. Bioeng. Biotechnol. 10 (2022) 1025155.
M. Naeem, W. Kim, J. Cao, et al., Colloid Surf. B: Biointerfaces 123 (2014) 271–278.
W. Li, Y. Li, Z. Liu, et al., Biomaterials 185 (2018) 322–332.
C. Abraham, R. Medzhitov, Gastroenterology 140 (2011) 1729–1737.
A. Geremia, P. Biancheri, P. Allan, et al., Autoimmun. Rev. 13 (2014) 3–10.
S. Zhang, R. Langer, G. Traverso, Nano Today 16 (2017) 82–96.
L.M. Hegarty, G.R. Jones, C.C. Bain, Nat. Rev. Gastroenterol. Hepatol. 20 (2023) 538–553. doi: 10.1038/s41575-023-00769-0
C. Danne, J. Skerniskyte, B. Marteyn, et al., Nat. Rev. Gastroenterol. Hepatol. 21 (2024) 184–197. doi: 10.1038/s41575-023-00871-3
X. Han, R. Luo, S. Qi, et al., J. Nanobiotechnology 21 (2023) 321.
J. Zhang, A. Ou, X. Tang, et al., J. Nanobiotechnology 20 (2022) 389. doi: 10.3390/toxins14060389
P. Diez-Echave, A.J. Ruiz-Malagon, J.A. Molina-Tijeras, et al., Int. J. Pharm. 606 (2021) 120935.
H. Wang, L. Wang, S. Guo, et al., ACS Appl. Mater. Interfaces 14 (2022) 26327–26337. doi: 10.1021/acsami.2c02295
J. Liu, Y. Bai, Y. Li, et al., Ebiomedicine 107 (2024) 105301.
T. Takiishi, C. Fenero, N. Camara, Tissue Barriers 5 (2017) e1373208. doi: 10.1080/21688370.2017.1373208
S. Citi, Science 359 (2018) 1097–1098. doi: 10.1126/science.aat0835
M. Schwarzfischer, G. Rogler, Metabolites 12 (2022) 223. doi: 10.3390/metabo12030223
Q. Shen, Z. Huang, J. Yao, et al., J. Adv. Res. 37 (2022) 221–233.
S. Qi, R. Luo, X. Han, et al., ACS Appl. Mater. Interfaces 14 (2022) 50692–50709. doi: 10.1021/acsami.2c17827
C. Guo, J. He, X. Song, et al., Pharmacol. Res. 149 (2019) 104463.
J. Feng, Y. Wang, Y. Lv, et al., Mol. Pharm. 19 (2022) 4157–4170. doi: 10.1021/acs.molpharmaceut.2c00550
Z. Zeng, Z. Xie, G. Chen, et al., Food Funct. 13 (2022) 649–663. doi: 10.1039/d1fo02702f
H. Han, L. Ke, W. Xu, et al., Food Funct. 14 (2023) 8420–8430. doi: 10.1039/d3fo00641g
B. Yilmaz, P. Juillerat, O. Oyas, et al., Nat. Med. 25 (2019) 323–336. doi: 10.1038/s41591-018-0308-z
M. Akhtar, Y. Chen, Z. Ma, et al., Anim. Nutr. 8 (2022) 350–360.
Z. Zhang, H. Zhang, T. Chen, et al., Cell Commun. Signal. 20 (2022) 64.
S. You, Y. Ma, B. Yan, et al., Front. Nutr. 9 (2022) 1000517.
X. Bai, Z. Feng, S. Peng, et al., Biomater. Adv. 139 (2022) 213002.
X. Li, Z. Duan, X. Chen, et al., Adv. Mater. 35 (2023) 2300548.
Y. Zhang, Z. Fang, D. Pan, et al., Adv. Mater. 36 (2024) 2401304.

Figure 1 The key features of colon-targeted NDDS. NDDS can be modified in various ways to surmount the hurdles associated with colon-targeted oral drug delivery.

 扫一扫看文章
扫一扫看文章

扫一扫关注我们
 DownLoad:
DownLoad:
 下载:
下载:

 下载:
下载: