Collaborative Innovation Centre of Regenerative Medicine and Medical BioResource Development and Application Co-constructed by the Province and Ministry, Guangxi Medical University, Nanning 530021, China
b.
Bioscience and Biomedical Engineering Thrust, Systems Hub, The Hong Kong University of Science and Technology (Guangzhou), Nansha, Guangzhou 511400, China
c.
Division of Life Science, The Hong Kong University of Science and Technology, Hong Kong 999077, China
d.
Department of Hematology, Department of Orthopedics, The Seventh Affiliated Hospital of Sun Yat-sen University, Shenzhen 518107, China
e.
Department of Orthopedics, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou 510120, China
junwuhkust@ust.hk (J. Wu). 1 These authors contributed equally to this work.
Received Date:
12 January 2025 Accepted Date:
25 March 2025 Revised Date:
24 March 2025 Available Online:
15 April 2026
Abstract:
Bone-related diseases resulting from accidents, illnesses, and injuries have become increasingly common in recent years. Treating these conditions poses significant challenges, including prolonged recovery times, high costs, and unpredictable outcomes, which can lead to complications such as infections and reduced muscle strength. Although autologous bone transplantation is regarded as the "gold standard" for addressing bone diseases, its application is often limited by complications at the donor site and the risk of infection. This underscores the urgent need to explore alternatives to autogenous bone transplantation. In response, a range of biomaterials for bone repair have been developed, with metal-based biomaterials emerging as effective adjuncts that enhance and optimize the repair and regeneration of bone tissue. These materials can actively influence the bone repair process through mechanisms such as inductive osteogenesis, immunomodulation, and pro-angiogenesis. This review begins by highlighting the biological effects of metal-based biomaterials, followed by a comprehensive overview of their macro- and micro-scale classifications and applications for treating various bone diseases. Finally, the review addresses future directions and challenges associated with the use of metal-based biomaterials in bone repair, aiming to propose promising strategies for the treatment of bone-related diseases.
Bone is one of the most critical organs in the human body, serving as a key component of the musculoskeletal system that provides structural support, protection, mobility, and hematopoiesis. The primary mineral component of bone is calcium phosphate [1], its remarkable feature lies in the deposition of a large amount of calcium salts in the extracellular matrix (ECM), forming a highly durable tissue that makes up the skeletal framework of the human body, providing support and protection to various organs [2]. However, numerous factors can cause bone defects or loss, including trauma, orthopedic surgery, osteoarthritis (OA) [3], osteoporosis, and resection of primary tumors [4,5]. Furthermore, with the rising number of patients owing to an aging population, the prevalence of bone diseases continues to increase annually. It is estimated that approximately 20 million patients worldwide suffer from bone tissue loss because of various ailments each year [6].
Generally, the human skeletal system has the capacity to regenerate in response to minor injuries or small bone defects [7]. However, when the defect surpasses a critical size threshold, the process of natural healing becomes significantly more difficult [8]. In cases of severe bone injury, the use of natural bone grafts or biomaterials is often essential to bridge the gap and support bone regeneration. Currently, bone grafting remains the standard method for repairing extensive bone defects, which includes autologous, allogenic, and xenogeneic grafting options [9–12]. Among these, autologous bone grafting is known for its excellent repair effects and remains as the "gold standard" owing to its osteoinductive, osteogenic, and osteoconductive characteristics [13]. However, the application of autologous grafts requires harvesting healthy bone tissue, which may be limited in availability, and the second surgical intervention may lead to complications, and inadequate defect filling [14]. Allogenic bone grafts, obtained from other patients or human donors, can help address the deficiency of autologous bone [15]. Unfortunately, these donor tissues carry risks of infection, disease transmission, and immune response [16]. As a result, researchers generally do not recommend the widespread use of these materials for bone defect repair [17]. Other standard treatments present limited selectivity for tumor cells and high toxicity to normal cells, further restricting their clinical application [18].
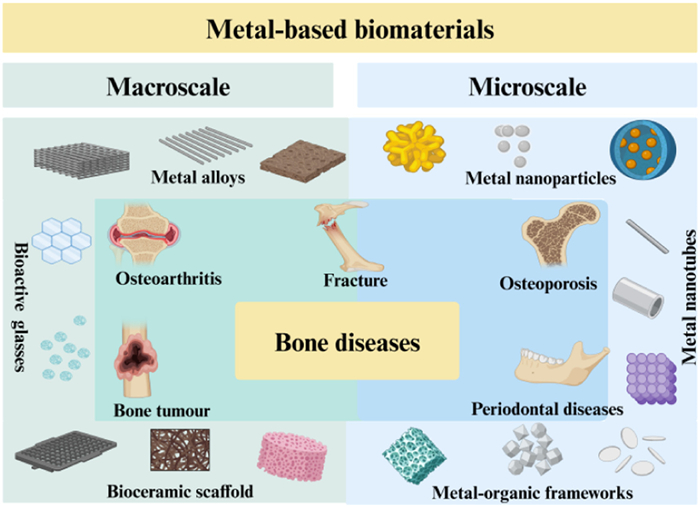
Given these challenges, there has been a significant demand over the past few decades for the rational design and construction of multifunctional biomaterials that facilitate disease treatment and bone regeneration [19]. In recent years, metal-based biomaterials have attracted considerable attention due to their outstanding mechanical strength and crucial role in promoting bone formation and regeneration [20]. Compared to traditional polymer and ceramic materials, metal-based biomaterials exhibit significant advantages in bone repair. For most metal materials, their superior mechanical properties provide high strength and excellent toughness, allowing them to effectively support biological loads and resist fatigue [21]. This remarkable mechanical strength ensures that metal implants maintain structural integrity in dynamic biological environments, facilitating load transfer during the bone healing process and enhancing tissue regeneration, Furthermore, the biocompatibility and corrosion resistance of metal-based biomaterials are crucial for their effectiveness in bone repair. These materials form favorable interfaces with surrounding bone tissue, which helps minimize inflammatory reactions. Their excellent corrosion resistance in physiological environments extends the lifespan of implants and reduces the risk of complications. Additionally, certain metals possess inherent antibacterial properties, significantly lowering the incidence of infections at the implant site. This is particularly vital in bone repair surgeries, as infections can not only delay healing but also lead to serious clinical consequences. Thus, the enhanced antibacterial performance of metal-based biomaterials represents a key advantage. Moreover, the processability of metal-based biomaterials allows for the fabrication of complex-shaped implants tailored to specific clinical needs. This versatility supports the advancement of personalized medicine and contributes to improved surgical outcomes. Current research in bone tissue engineering increasingly emphasizes enhancing the biological activity of these materials through a range of physical and chemical surface modifications [22,23]. However, the classification of these metal-based materials for bone repair remains unclear. Bone regeneration is a complex process that requires the coordinated regulation of osteogenesis, immune responses, and the biological behaviors of the involved biomaterials. Recognizing that different metal-based materials play distinct roles in osteogenesis shaped by their structural characteristics, material morphology, and surface coatings, this review classifies these materials on both macro- and microscales. It emphasizes the biological effects of metal-based biomaterials and summarizes their biological characteristics and applications in treating bone diseases. Additionally, the review addresses current challenges and issues faced by metal-based biomaterials in bone repair and discusses future development directions. The aim is to propose promising strategies for the effective treatment of bone-related diseases (Fig. 1).
Figure 1
Figure 1.
Classification diagram of metal-based biomaterials utilized for common bone-related diseases. The macroscale classification comprises metal alloys, Bioactive glasses, and bioceramic scaffolds. The microscale classification includes metal nanoparticles, metal nanotubes, and metal-organic frameworks.
2.
Biological effects of metal-based biomaterials for bone regeneration
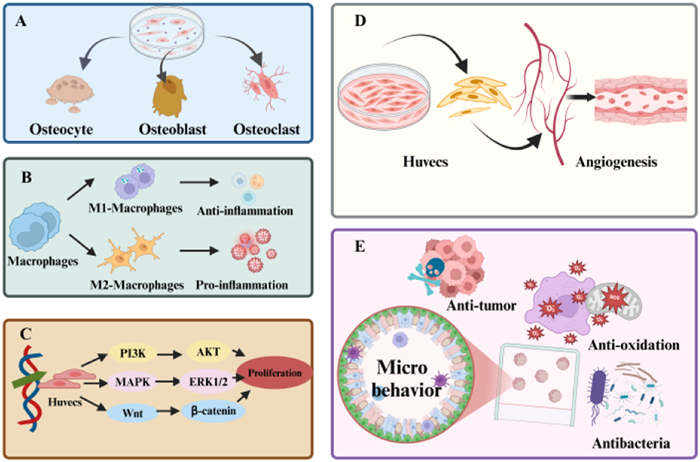
Bone tissue is a complex system predominantly composed of cells and ECM. The cellular components include mesenchymal stem cells (MSCs), progenitor cells, osteoblasts, osteoclasts, nerve fibers, endothelial cells from the circulatory system, and immune cells. The ECM is crucial as it provides essential nutrients and space for cellular proliferation, while also facilitating the removal of metabolic waste. Additionally, intricate metabolic activities occur during both physiological homeostasis and pathological disturbances within bone tissue. Regulating these metabolic processes is vital for promoting effective bone regeneration (Fig. 2). Metal-based biomaterials can enhance metal immunotherapy through unique biological effects, stimulating a series of mechanical effects that accelerate bone healing. During the tissue repair process, hypoxia and inflammation induce angiogenesis. The cells surrounding the blood vessels differentiate and proliferate in response to hypoxia, filling the wound while upregulating osteogenic genes and inducing the expression of relevant factors. This activates signaling pathways that promote bone healing, responding to growth factors released by platelets, inflammatory cells, and adjacent tissues, ultimately enhancing the stability of bone formation. Simultaneously, the complex molecular mechanisms that underline these strategies are being actively investigated, while the rapid advancement of biomaterials expands the potential applications of metal-based materials in bone regeneration.
Figure 2
Figure 2.
Schematic diagram of biological effects of metal-based materials. (A) The functional regulation of osteoblasts and osteoclasts. (B) Modulating the inflammatory response to establish a supportive immune microenvironment for bone. (C) Upregulation of osteogenic genes and activation of signaling pathways. (D) Promoting angiogenesis in new bone formation. (E) Other biological effects (such as anti-tumor, antioxidant, and antibacterial).
2.1
Induction of osteoblast differentiation, proliferation, and adhesion
Metal-based implants can induce the differentiation, proliferation, and adhesion of cells. The primary cells involved in bone remodeling are osteoblasts and osteoclasts. Following the implantation of metal-based biomaterials, the functions of these cells are closely interconnected, promoting the resorption of damaged bone and the formation of new bone. Additionally, osteocytes serve as mechanical sensors and play a crucial role in bone remodeling by initiating the process through matrix degradation [24]. Chondrocytes expand cartilage through proliferation and mesenchymal formation. From the tips of bone formation to the diaphysis, osteoblasts, vascular cells, osteoclasts, and other hematopoietic cells undergo widespread differentiation and proliferation. Notably, hypertrophic chondrocytes are crucial factors and regulators of bone growth [25]. The implanted metal-based biomaterials provide a scaffold for osteoblasts, allowing them to invade cartilage and blood vessels, forming true bone matrix in cartilage and generating primary trabecular tissue. Concurrently, metal-based materials can produce bioactive factors, and important osteogenic molecules are expressed in the periosteum, regulating the transformation and maturation of cells into osteoblasts through various pathways.
2.2
Activation of the immune system
For most metal-based implants, particularly those involving metal ions, the active ions they carry can activate the immune system, providing a suitable cellular microenvironment for bone repair. Their surface structures influencing cell adhesion and migration enhance local immune responses. With the awareness of the role of metal-based materials in immunotherapy deepens, it is recognized that the degradation or corrosion of these materials within the body can release metal ions (such as zinc (Zn), Cu, and Ag), which directly influence immune cell functionality. For instance, Zn2+ has been shown to enhance T cell proliferation and activity, while certain metals like Ag exhibit antibacterial properties that inhibit bacterial growth and reduce infection risks [26]. This characteristic contributes to an improved local immune environment and mitigates inflammation. Furthermore, some metal materials, as they degrade, can release bioactive substances that promote tissue regeneration and activate the immune system by stimulating osteoblasts and other immune cells [27]. Notably, studies have suggested that metal materials undergoing surface modification or specific treatments can induce immune tolerance and diminish rejection reactions to implants. Metal-based biomaterials activate the immune system through a variety of mechanisms, facilitating tissue repair and regeneration. Luo et al. introduced the term "metal immunology" in 2020 [28], while Wang et al. proposed the concept of "metal immunotherapy for cancer" in 2022, which garnered widespread attention [29]. This evidence underscores the relatively low side effects of metal-based materials and their feasibility in accumulation processes, suggesting their unique advantages in immunotherapy.
2.3
Activation of osteogenic related signaling pathways
Research has shown that metal-based materials can regulate the osteogenic differentiation of stem cells through the activation of specific signaling pathways and transcription factors, thereby promoting bone repair. Trabelsi et al. [30] proposed that Ti-Ag nanoparticles (NPs) can enhance the osteogenic differentiation of bone marrow-derived mesenchymal stem cells (BMSC) is facilitated by the activation of the mitogen-activated protein kinase (MAPK)/extracellular regulated protein kinases (ERK) signaling pathway. Thanks to the similarities in mechanical properties, biocompatibility, and biodegradability of Zn-based biomaterials with bone, Zhu et al. [31] investigated the biological response of human BMSC to Zn, focusing on the potential cellular signaling mechanisms involved. The findings demonstrated that Zn2+ activates the cAMP-PKA pathway, induces intracellular Ca2+ responses, and leads to MAPK activation, which elucidates the cellular signaling mechanisms by which zinc induces bone formation. Alotaibi et al. [32] certified that the activation of the osteogenic gene ERK1/2 pathway significantly participates in the osteogenic differentiation of BMSC and is activated by the implantation of Ti with nano-form Sr, Zn, and silicon (Si) bioactive ions. He et al. [33] prepared magnesium (Mg), Zn, and Mg-Zn mixed extracts to study their specific effects on the osteogenic differentiation of human BMSC and the MAPK signaling pathway. The results indicated that both Mg and Mg-Zn mixed extracts significantly promoted the osteogenic differentiation of human BMSC. Yunok et al. [34] also applied a Watmann protein-specific inhibitor to magnesium-pretreated BMSC. The cell density and activity were significantly reduced, while alkaline phosphatase activity and matrix mineralization were inhibited. These findings suggest that Mg2+ can enhance the expression of osteogenic markers, including alkaline phosphatase and bone morphogenetic proteins (BMPs), through the activation of the phosphatidylinositol-3-kinase/protein kinase B (PI3K/Akt) pathway, generating a series of changes in bone metabolism [35]. Li et al. [36] developed a novel ZA-CaP bilayer coating on Mg-Sr alloys through chemical deposition. Quantitative real-time polymerase chain reaction (PCR) and Western blotting results indicated that ZA-CaP double-coated Mg-Sr alloys regulate the formation of osteoblasts and osteoclasts through estrogen receptor α and nuclear factor κB signaling pathways. Consequently, metal ions may offer more direct therapeutic signals for promoting bone regeneration.
2.4
Stimulation of angiogenesis
The metallic mediators exert their effects through pathways involving vascular endothelial growth factor (VEGF), hypoxia-inducible factors (HIFs), angiogenesis-related genes, and immunomodulation of macrophages, thereby regulating angiogenesis. The presence of abundant vasculature in bone is crucial for bone regeneration [37]. In the research conducted by Chen et al., the implantation of VEGF-doped metallic scaffolds into rat cranial defects gave rise to a threefold increase in angiogenic capacity. Furthermore, the addition of VEGF enhanced scaffold functionality by 30%, significantly increasing overall bone density and promoting bone repair [38]. Zhou et al. also confirmed that BG and VEGF-coated scaffolds showed good outcomes in bone regeneration and defect healing in severe bone defect models in rats [39], exhibiting higher total bone formation, neovascularization, and bone regeneration. This evidence underscores the importance of directly incorporating angiogenesis-related genes into metal implant materials for angiogenesis and bone integration. Therefore, in studies without angiogenesis-related gene incorporation, Wang et al. found that under the controlled release of metal scaffolds, bioactive factors are essential for promoting angiogenesis and ensuring cell survival, migration, nutrient delivery, and the diffusion of bone and angiogenic factors in vivo [40].
2.5
Other effects
Years of research and applications have confirmed that various metals and alloys also exhibit strong antibacterial activity, such as Ag and its alloys, Cu and its alloys, Zn oxide, Ti oxide, and Mg. In the bone regeneration system, these metal ions suppress bacterial growth and inflammation, further promoting bone repair effects. Furthermore, modified metal-based materials contain immunomodulators that can activate immune cells to regulate the tumor microenvironment and enhance anti-cancer immunity [41].
3.
Different types of metal-based biomaterials
Metal-based materials have become a central focus of research in bone repair due to their outstanding mechanical properties, biocompatibility, and customizable surface characteristics. With the aging population and the rising incidence of bone-related diseases, the demand for effective bone repair solutions has become more urgent. Various surface modification techniques, such as coatings, surface roughening, and bioactive coatings. Significantly enhance the interaction between these materials and the surrounding bone tissue. These modifications facilitate the adhesion, proliferation, and differentiation of bone cells, thereby accelerating the bone regeneration process. Furthermore, metal-based materials can influence the microenvironment of bone tissue by releasing bioactive factors, further promoting the repair process. However, the effectiveness of different metal-based materials in supporting bone repair can vary widely based on factors such as size, material structure, modification methods, synthesis processes, and degradation rates. We classify and examine the most commonly used metal-based bone repair materials from both macro- and microscale perspectives, focusing on their structural scale, implantation methods, and mechanisms of action, emphasizing their distinctive characteristics and applications.
3.1
Macroscale metal-based biomaterials
Metal-based biomaterials with macroscales typically consist of micro-sized or larger scale, often fabricated into specific shapes such as scaffolds, implants, or surgical instruments. These materials are designed for direct contact with bone tissue or other biological tissues and possess excellent mechanical strength and corrosion resistance, enabling them to withstand the internal loads and chemical environments within the body. Additionally, significant differences in elastic modulus and tensile strength between metal and bone can lead to stress shielding, potentially weakening the surrounding bone structure. Once a fracture has healed, these macroscopic implants often necessitate invasive secondary surgery for removal. To minimize patient trauma and reduce medical costs, biodegradable implants are emerging as a viable alternative to traditional metal implants [42–44]. This section provides an overview of common macroscopic metal implants used in orthopedics, focusing primarily on metal alloys, bioactive glass (BG), and bioceramic scaffolds.
3.1.1
Metal alloys
Metals and their alloys are increasingly recognized as effective biomaterials for bone repair, primarily due to their exceptional mechanical strength and fracture toughness. Traditional materials, such as stainless steel and Ti alloys, offer excellent mechanical properties that support bone growth. However, their high elastic modulus can lead to significant stress shielding effects, and patients often require a second surgery to remove these implants. Considering these challenges, biodegradable metals have emerged as promising alternatives, effectively addressing the limitations of conventional alloys. Consequently, they are rapidly becoming a focal point of research in the field of biomedical materials (Fig. S1 in Supporting information). An ideal biodegradable metal for bone repair should gradually dissolve after the healing process, leaving no residual material in the body [45].
Promising candidates for this application include Fe, Mg, Zn, and their alloys, as they possess the ability to degrade progressively. Current research is particularly concentrated on Fe and Mg-based alloys. Fe and its alloys are known for their excellent mechanical properties, although they are prone to oxidation in humid environments (Fig. S1A) [46]. While Fe-based alloys achieve a favorable balance between mechanical strength and biocompatibility, their relatively slow degradation rate presents significant drawbacks. As a result, researchers are increasingly exploring Mg alloys (Fig. S1B). Mg and its alloys closely resemble the density and elastic modules of natural bone, making them suitable as temporary implants that completely degrade post-healing [47]. However, pure Mg metal degrades too rapidly for direct use. To optimize Mg for bone repair, researchers have investigated ternary alloys containing elements such as Mg-Zn-Sr or Mg-Zn-Ca, the incorporation of these elements can enhance both mechanical properties and degradation rates. Furthermore, Mg alloys have demonstrated strong anti-infective effects against common orthopedic pathogens due to their degradation in bodily fluids.
While Zn-based alloys exhibit a moderate degradation rate compared to Fe and Mg alloys, their lower strength and elastic modulus limit their applicability [48,49]. To address this, various alloying elements have been introduced to develop Zn alloys with tailored properties [50]. Additionally, Ti and its alloys are widely regarded as excellent materials for bone implants due to their corrosion resistance, relatively low elastic modulus, and low density (Fig. S1C). Nonetheless, the limited mechanical and physicochemical properties of these alloy materials continue to pose challenges in treating bone diseases. Future research should prioritize the combination of these materials with various components to impart multifunctional properties, thereby addressing their shortcomings in bone repair and enhancing their clinical applications.
3.1.2
BGs
BG establishes a robust biological connection with both soft and hard tissues, thereby minimizing the risk of infection following implantation during bone reconstruction. As a result, it is commonly utilized as a bone filler or graft material [51].
A notable feature of BG is its ability to incorporate metal ions-such as Sr, Cu, Zn, and fluorine-into its structure. Osteoblasts cultured on the surface of titanium-doped BG show a higher proliferation rate compared to those on 45S5 BG, attributed to the more controlled release of soluble components. Even small amounts of Sr2+ have been shown to enhance bone structure stability [52], stimulate osteoblast activity, reduce osteoclast activity [53], and promote new bone tissue formation. Zn and Cu impart anti-inflammatory properties to BG [52], allowing it to function as a therapeutic anti-inflammatory agent [54,55]. Additionally, these ions contribute antibacterial properties to BG coatings. The inclusion of zinc improves the chemical stability and mechanical properties of BG [56], while Mg2+ enhances its biological activity. Mg2+ increases the solubility of BG but decreases the crystallization rate of hydroxyapatite on its surface [57]. The incorporation of Mg particles has also been shown to improve the mechanical properties of BG [58]. Bi2+ doping can yield biocomposite materials with photothermal effects, maintaining biocompatibility and remineralization properties akin to hydroxyapatite, while reducing the number of treatment cycles needed to heal bone defects. Ta doping results in cell-compatible materials with enhanced biological activity and strength [59]. Ta-doped BG cements exhibit favorable rheological properties, hardness, radiation impermeability, and antibacterial effects, making them suitable for applications such as sternum fixation [60]. Aluminum (Al) increases the density and microhardness of BGs with high phosphorus content due to the formation of PO-Al bonds. Notably, the 6% Al content significantly enhances biological activity and cell proliferation rates [61]. Niobium-doped 45S5 BG shows improved bioactivity [62], while the addition of Fe3+ and Co2+ brings greater density and compressive strength, enhancing the biological function of BG and promoting bone formation [63]. Moreover, elements like Si, Ca, and phosphorus (P) released from BG can activate signaling pathways that mediate the differentiation of bone marrow mesenchymal stem cells into osteoblasts, thereby promoting bone tissue regeneration and repair.
Despite significant advancements, further research is essential to enhance the mechanical properties of BG for the effective repair of larger bone tissue defects in vivo. Additionally, aligning the degradation rate of BG with the pace of new bone formation, as well as improving repair efficiency and reducing costs, remains a critical area for future investigation [64]. Some common macroscale metal-based materials aforementioned are summarized in Table 1 [46–49,54,55,57,59–63,65].
Table 1
Table 1.
The typical examples of metal alloys and BGs for the treatment of bone disease.
Bioceramic scaffolds play a vital role in providing mechanical support by resisting external stress and maintaining the shape and integrity of tissues. They are biocompatible materials that can be accepted by the human body without adverse effects, while also promoting interaction with surrounding tissues to facilitate growth [66]. Biologically used inert ceramics in research include alumina (Al2O3) [67], Ti dioxide (TiO2) [68], zirconia (ZrO2), zinc oxide (ZnO) [69], and silicon nitride (Si3N4). These bioceramics are biologically active or bioabsorbable, meaning they can trigger chemical and biological responses in the physiological environment, thereby promoting bone growth and repair. Most porous bioceramic scaffolds enhance cell migration and proliferation, improve the transport of nutrients and metabolites, and facilitate bone integration and vascular reconstruction [70]. Additionally, these scaffolds can release bioactive substances that stimulate cell proliferation and differentiation, ultimately supporting bone repair. Among biodegradable bioceramic materials, scaffolds doped with Mg2+ have demonstrated superior degradation and osteogenic effects in vivo. It is important to note that high concentrations of Mg2+ can exhibit cytotoxicity and inhibit new bone formation [71]. To create a highly uniform CaSiO2 scaffold with a pore-controlled structure and excellent mechanical properties, Wu et al. successfully utilized 3D printing technology prepared this scaffold. The results demonstrated that the CS scaffolds exhibited not only outstanding compressive strength but also satisfactory apatite mineralization capabilities and a high level of bone defect healing, indicating that 3D-printed CS scaffolds hold significant potential for bone tissue regeneration [72]. Similarly, Zhu et al. developed a Sr-containing bioceramic scaffold and found that it significantly promoted the proliferation of rBMSCs, increased alkaline phosphatase (ALP) activity, and elevated the expression of osteogenic-related genes [73]. Additionaly, Deng et al. prepared a Mg-doped bioceramic scaffold, which proved effective in regenerating cartilage and subchondral bone tissue. This efficacy is primarily attributed to the synergistic effects of the metal ions released by the scaffold, which significantly stimulate chondrocyte maturation and cartilage regeneration [74].
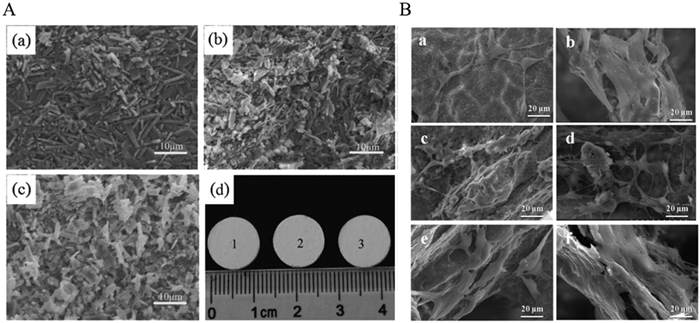
Despite their advantages, bioceramic scaffolds used as implant materials in bone regeneration engineering pose a risk of infection. Drug therapy is typically employed to manage associated infections. To achieve localized and targeted therapeutic effects, researchers such as Unnithan et al. have introduced antibiotics or other drugs into bioceramic scaffolds, controlling their structural characteristics to enhance efficacy [75]. Radmansouri et al. prepared Mg-Ca-Ti-dioxide scaffolds loaded with doxycycline, demonstrating excellent drug release capabilities, biological activity, and antibacterial efficacy [76]. The combination of metal-loaded bioceramic scaffolds with antibiotic strategies can yield a dual benefit: promoting bone repair while preventing implant infections. This approach is increasingly favored for clinical applications. Therefore, bioceramic scaffolds can be partially or completely absorbed by the human body without associated infection risks, underscoring their advantages over metal scaffolds in various medical applications (Fig. 3) [77].
Figure 3
Figure 3.
(A) SEM images and photos of calcium sulfate based composite bioceramic bone cement: (a) Calcium sulfate, (b) 15% by weight mesoporous magnesium silicate, (c) 30% by weight mesoporous magnesium silicate, (d) photos of bone cement. (B) SEM images of bioceramic scaffolds on cell morphology: (a, b) 45S5 BG scaffold, (c, d) drug free chitosan PVP-45S5 Bioglass bone scaffold, and (e, f) vancomycin loaded chitosan/PVP-45S5 Bioglass bone scaffold. Reproduced with permission [77]. Copyright 2024, Elsevier.
Due to limited corrosion resistance, low cell proliferation rates, and bacterial adhesion associated with traditional orthopedic implants, complications and implant failures have frequently been reported [78]. The demand for advanced materials in orthopedic applications is on the rise. In addition to the aforementioned macroscale metal-based biomaterials, recently microscale metal-based biomaterials might offer innovative solutions to the challenges faced by the orthopedic industry, generating significant interest. Most metal-based biomaterials with microscales consist of nanoscales, including NPs, thin films, or other microstructural forms. They exhibit superior physical, chemical, and mechanical properties compared to traditional materials, with a strong focus on surface characteristics such as biocompatibility, antibacterial properties, and cell adhesion, making them ideal for integration into orthopedic implants and scaffolds. As a result, metal-based biomaterials with tailored microstructures are emerging as promising candidates for tissue engineering scaffolds, ushering in a new era in this field [79].
3.2.1
Metal NPs
Benefited from the nanoscale size, high surface area-to-volume ratio, and distinctive physical and chemical properties, metal NPs have become promising candidates for producing tissue engineering scaffolds [63]. Compared with traditional biomaterials, metal NPs can significantly enhance cell growth and facilitate the repair of bone injuries. Their superior properties enable them to deliver bioactive molecules, control nutrient acquisition, and improve the adhesion performance of cell implantation scaffolds. The unique characteristics of metal NPs have opened new avenues in bone tissue engineering [80]. Commonly studied metal NPs include gold (Au), Ag, Fe, Al, Cu, Zn, and Mg, most of which are recognized for their excellent antibacterial properties and adjustable mechanical characteristics. Although some metal NPs can induce apoptosis or trigger reactive oxygen species (ROS) and DNA damage, it has been established that, when appropriately sized and dosed, most metal NPs are beneficial.
(1) AuNPs: In recent decades, AuNPs have gained prominence in bone tissue engineering profiting from their low toxicity, antibacterial activity within scaffold microenvironments, and high biocompatibility [81]. AuNPs are recognized as novel osteogenic agents capable of inducing the osteogenic differentiation of stem cells through various signaling pathways, including the Wnt/β-catenin, ERK/MAPK, and p38/MAPK pathways [82,83]. Amorosa et al. [12] developed an injectable hydrogel system incorporating functionalized AuNPs to enhance bone differentiation, confirming both the biocompatibility of AuNPs and their osteogenic potential. Similarly, Heo et al. [84] integrated AuNPs into Ti implants, proving that these NPs can significantly enhance bone integration in vitro. Furthermore, Amina et al. highlighted the ability of AuNPs to carry various therapeutic agents, including drugs, peptides, proteins, DNA, and RNA, suggesting their potential for advancements in molecular diagnosis and nanotherapy in bone-related research [85]. However, Jia et al. [86] reported that AuNPs with sizes ranging from 1 to 2 nanometers exhibited acute toxicity to various cell lines, indicating that cellular uptake could lead to apoptosis or necrosis and potential accumulation in organs.
(2) AgNPs: AgNPs could be found in diverse fields, including coatings and tissue regeneration, owing to their potent biological properties [87]. Numerous studies have revealed that AgNPs possess antibacterial properties, making them ideal candidates for wound dressings and bone substitutes. Xu et al. [88] observed that during the repair of bone-related conditions, only Ag+ are released to target bacterial infections. Meanwhile, Prabhu et al. [89] found that AgNPs can infiltrate bacterial cells, leading to damage of the cell membranes and subsequent cell death. Vadakkan et al. [90] observed that treating Escherichia coli and Staphylococcus aureus with AgNPs could lead to cell surface damage and significant ROS production, thus inhibiting bacterial growth. However, AgNPs can also cause harm to human cells, including ROS [91] generation and DNA damage [92]. The toxicity of AgNPs is influenced by factors such as particle size, morphology, surface chemistry, aggregation level, and dosage. Research has shown that loading AgNPs onto various carriers can mitigate their toxicity. Gao et al. [93] incorporated Ag oxide NPs into Ti oxide nanotubes, obtaining a structure that exhibited improved cell compatibility and reduced toxicity, while promoting osteoblast proliferation and differentiation. Sun et al. [94] created an innovative collagen scaffold that encapsulates silver NPs along with BMP-2, illustrating enhanced antibacterial activity. This study indicated that, although Ag exhibits cytotoxicity above a certain threshold, controlled release of an appropriate amount of Ag can achieve antibacterial effects without harming surrounding tissues [90,95]. Additionally, Nandi et al. [96] reinforced the adhesion of AgNPs through heat treatment, showcasing a promising approach for the treatment of osteomyelitis.
(3) AlNPs: Al is a biologically inert metal and serves as an essential element for life. However, AlNPs have been applied broader in orthopedic implants than Al itself. Research indicates that modified alumina materials, particularly those treated with porous ceramic coatings, exhibit favorable bone integration properties, and can help to mitigate the risk of long-term implant failure. Hasan et al. discussed how AlNPs can adhere to bacterial cell walls, deform them, and ultimately lead to cell death, thus causing their antibacterial properties [97,98]. Yu et al. [99] illustrated that the presence of Al2O3 contributes to the formation of interconnected microporous scaffolds, which are vital for cell adhesion, nutrient transport, and proliferation, thereby improving the mechanical and biological properties of various bone scaffolds. Derazkola et al. [100] found that incorporation of AlNPs into PMMA nanocomposites improved their physical properties, such as hardness, flexural strength, and tensile strength. Similarly, Farjaminejad et al. [101] explained that AlNPs increased the mechanical strength of β-tricalcium phosphate (β-TCP) scaffolds while promoting alkaline phosphatase production and calcium phosphate deposition. However, alumina NPs may exhibit toxicity, as Hashimoto et al. observed their cytotoxicity and genotoxicity associated with ion release [102,103]. Zhang et al. [104] noted that AlNPs can enter cells and induce ROS production, raising potential toxicity concerns. AlNPs serve as effective reinforcing agents for scaffolds, enhancing their physical, chemical, mechanical, and biological properties but still presenting cytotoxicity challenges.
(4) CuNPs: CuNPs have attracted interest in bone tissue engineering due to their distinctive antibacterial properties and their capacity to promote collagen fiber deposition and angiogenesis. Eivazzadeh-Keihan et al. noted that Cu supplementation in biomedical studies is associated with a decrease in bone mass and mechanical strength, suggesting that Cur is critical in bone formation [105]. Recent studies have highlighted the potential of CuNPs as novel bone substitutes. The large surface area to volume ratio of Cu allowed it as a promising antibacterial agent [53] and a candidate for treating osteoporosis [106]. Sahmani et al. [107] enhanced the mechanical properties and cell viability of hydroxyapatite (HA) scaffolds by incorporating copper oxide NPs. Despite their positive charge attributes in biomedical applications, CuNPs have been linked to strong inflammatory responses and cytotoxicity. To deal with these concerns, researchers have explored coating CuNPs with biocompatible materials, such as natural and synthetic polymers, to create novel nanocomposites. Tabesh et al. [108] integrated chitosan with CuNPs to create an antibacterial coating, exhibiting the optimal antibacterial efficacy against both Gram-positive and Gram-negative bacteria. Hengel et al. [109] functionalized bone implants with varying percentages of silver and CuNPs to enhance their antibacterial and bone-conducting properties. Collectively, these studies indicate that composite nanosystems incorporating CuNPs can enhance the mechanical properties of nanocomposites used in bone tissue engineering, while providing antibacterial and therapeutic benefits for osteoporosis.
(5) ZnNPs: Zn is a crucial element found in all biological tissues, where it plays a significant role in bone mineralization, contributes to cell membrane integrity, and facilitates pathological calcification [110]. Previous research has shown that Zn enhances cellular compatibility [111]. Afshar et al. [112] utilized Zn silicate mineral NPs on the surfaces of nanofiber scaffolds, resulting in improved cell compatibility and promoting both stem cell proliferation and osteogenic differentiation. Zhang et al. [113] developed a metal-polyphenol network (MPN) coating composed of protocatechuic acid and Zn ions (PCA+Zn2+), proving its potential as an innovative bone membrane with excellent biocompatibility and the ability to regulate oxidative stress. Hu et al. [114] reported that Zn-doped Ti dioxide coatings exhibited antibacterial properties, promoting the adhesion, proliferation, and differentiation of rBMSCs. However, He et al. [115] cautioned that Zn-doped coatings can generate ROS, inducing damage to bacteria through contact killing, while released Zn2+ may inhibit the growth of planktonic bacteria. Kononenko et al. [116] illustrated similar concentration-dependent cytotoxicity across all tested Zn compounds, confirming that Zn oxide NPs have the potential to induce genotoxic effects and interfere with cellular defense mechanisms. ZnNPs are frequently integrated with other biomaterials to achieve a diverse array of properties, including antibacterial efficacy, cell compatibility, and corrosion resistance [117]. Conversely, excessive exposure to Zn can cause cell apoptosis or necrosis [118].
(6) MgNPs: Mg is an essential element for human health [119], exhibiting several unique properties, including osteogenic stimulation, biocompatibility, and biodegradability. Compared to other metals, Mg possesses a lower Young's modulus [120], this increases the potential applications of MgNPs in orthopedic implants and scaffolds. In bone engineering, magnesium predominantly plays a significant role in the form of oxides. Mg oxide NPs are often used in combination with hyaluronic acid in bone substitutes [121]. Nogueira et al. [103] created a porous sodium alginate scaffold incorporated with Mg oxide NPs, significantly enhancing the scaffold's mechanical strength and antibacterial capabilities. Similarly, Dietler et al. [122] incorporated MgNPs into BG-based scaffolds to improve their biological behavior and antibacterial effects. Thus, MgNPs are widely utilized primarily because of their advantageous mechanical properties and antibacterial efficacy. However, Ghobadian et al. [123] reported that varying concentrations of Mg oxide NPs can induce cell apoptosis, DNA damage and the production of intracellular ROS.
The types of metal NPs mentioned are mainly summarized in Table S1 (Supporting information). This mainly summarizes their unique advantages, potential problems, applications forms, and therapy effects.
3.2.2
Metal nanotubes
Metal nanotubes have emerged as a promising platform for bone regeneration thanks to their superior biological properties, including geometric shape, porosity, chemistry, and biocompatibility [124]. Carbon nanotubes are known for their highly stable physical and chemical properties, which contribute to their potential in promoting the attachment and proliferation of osteoblasts, as well as the differentiation of mesenchymal stem cells [125]. However, the toxicity of carbon nanotubes upon entering the human body raises concerns, possibly due to the production of ROS, which can damage cells [126]. Beyond carbon nanotubes, a variety of materials-including metals, metal oxides, metal sulfides, and metal-organic frameworks (MOFs) can form tubular nanostructures under specific conditions [127]. These materials are progressively being applied in the field of bone regeneration. Metal nanotubes have shown broad application prospects in the field of drug delivery, bone repair, gene transfer, and cell isolation. This section primarily focuses on the applications of metal nanotubes and metal oxide nanotubes in bone repair engineering.
(1) Single metal nanotubes
Recently, the use of metal nanotubes in bone tissue engineering has advanced significantly. The surface morphology of these nanotubes plays a vital role in promoting bone integration by affecting the adhesion, shape, proliferation, and differentiation of osteogenic cells [126]. Ti nanotubes are the most widely utilized metal nanotubes for treating bone diseases, typically prepared via electrochemical oxidation. Research has shown that Ti nanotubes (TNT), benefiting from their nanoscale and physicochemical properties, can mimic the layered structure of natural osteogenic tissue. This indicates that TNT can facilitate the differentiation of mesenchymal stem cells into osteoblasts [128,129]. Based on this, to further explore cellular behavior and tissue response related to Ti nanotubes in bone repair, Huang et al. [130] proposed that the osteogenic process on TNT is related to the cytoplasmic transport of YAP, which reduces the likelihood of YAP/Runx2 binding and enhances the repair of bone-related conditions. Although research on single metal nanotubes in bone diseases is limited, the combination of two or more metals to create composite metal nanotubes presents a promising strategy for inducing new bone formation and achieving tighter bone integration [131]. Studies have shown Mg-doped nanotubes on Ti implants [132], suggest that these bifunctional Mg-doped Ti nanotubes effectively combat bacterial infections and mitigate bone resorption. Gérard et al. proved that Sr-cobalt metal composite nanotubes stabilize HIF-1α, activate the target gene VEGF, and enhanced bone integration around implants. However, excessive incorporation of metal nanotubes can lead to cytotoxicity. Similarly, Ta, another valve metal with excellent biocompatibility, outperforms titanium in terms of bone integration and corrosion resistance [133]. Wang et al. proposed that Ta nanotubes (Ta NT) can enhance protein adsorption, stimulate osteoblast activity, and promote early bone integration through implant interlocking [134]. Based on the previous research, Wu et al. [135] successfully modified titanium substrates with Ta-NT and Ta-Cu NT coatings through magnetron sputtering and anodizing techniques. Their study indicated that Ta-Cu NT, as a novel Ti-based implant delivery system, combines the beneficial properties of multiple metallic elements, improving antibacterial, angiogenic, and osteogenic effects.
In summary, while there is limited research on single metal nanotubes for bone diseases, composite metal nanotubes can effectively prevent bone infections and osteolysis, enhance antibacterial activity, promote angiogenesis, and present favorable therapeutic effects in bone-related conditions.
(2) Metal oxide nanotubes
Metal oxide nanotubes can significantly enhance the adhesion and proliferation of mesenchymal stem cells, with varying effects depending on their diameters and lengths [136]. Among metal oxide nanotubes, Ti dioxide nanotubes are the most prevalent. Most studies utilized Ti surface-prepared metal oxide nanotubes via anodic oxidation etching, significantly enhancing the differentiation of bone marrow mesenchymal stem cells into osteoblasts [137].
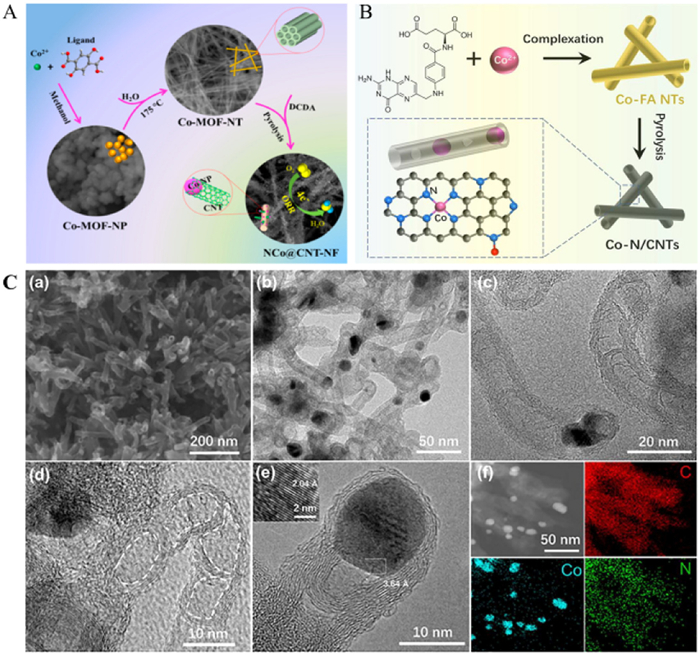
An additional advantage of Ti dioxide nanotubes is their open geometric structure at one end, which allows them to serve as potential carriers for bioactive agents [138]. Furthermore, metal NPs such as Ag, Sr, and Zn have been incorporated into Ti dioxide nanotubes to enhance the implant bone integration [139]. Yan et al. [140] prepared Mg2+-doped Ti dioxide nanotube arrays on Ti surfaces through electrochemical anodization and hydrothermal treatment, promoting the proliferation and differentiation of bone-forming cells. The incorporation of Mg into the nanotubes as Mg-TiO3 accelerated the proliferation of BMSCs on the surface of the MgNT. Moreover, Cheng et al. [141] created Ca-doped TiO2 nanotube films through anodic oxidation and hydrothermal treatment, indicating that the nanotube structure remained intact, effectively enhancing the adhesion, diffusion, and proliferation of osteoblasts in vitro. In a similar vein, Pan et al. [142] prepared Sr/Ag-doped Ti dioxide (TiO2) nanotube arrays on Ti surfaces, highlighting the osteogenic behavior, biocompatibility, and antibacterial activity of these composite nanotubes through ultraviolet (UV) irradiation. In a departure from traditional methods, Wang et al. [143,144] reported the first cobalt (Co)-doped single crystal MOF nanotube (Figs. 4A and B), presenting a new strategy for manufacturing MOF nanotubes and related one-dimensional metal nanostructures, serving as an inspiration for bone-related disease repair strategies.
Figure 4
Figure 4.
(A) Schematic diagram of synthesis of single-crystal Co-MOF nanotubes. Reproduced with permission [144]. Copyright 2018, American Chemical Society. (B) Schematic illustration for the synthesis and structure of Co2+ doped single crystal MOF nanotubes. (C) The morphology and elemental mapping characteristics of Co-N/CNTs are presented: (a, b) SEM images depict the surface structure. (c–e) HRTEM images provide detailed insights into the internal features. (f) EDS elemental images illustrate the elemental distribution within the Co-N/CNTs. The illustration in (e) highlights the high-resolution lattice structure of CoNPs. Reproduced with permission [143]. Copyright 2021, Elsevier.
Qiao et al. found that Sr-doped TiO2 (SrTiO3) nanotubes can significantly increase the expression of osteoblast-related genes during the osteogenic process, independent of osteogenic differentiation factors [145]. Escobar et al. [146] introduced lanthanum into the biological interface of SrTiO3 nanotubes (LSTN), and the obtained metal composite oxide nanotubes exhibited excellent hydrophilicity and protein adsorption capabilities, which are critical for osteoblast adhesion to the nanotube surface. Remarkably, LSTN certified no cytotoxicity while promoting bone cell proliferation and differentiation. Si, recognized as a vital trace element for human bone and cartilage growth, has also been incorporated into biomaterials or coatings to promote the proliferation and differentiation of osteogenic cells [147]. Carvalho et al. explained that Si-doped TiO2 films/coatings exhibit osteogenic and angiogenic properties, attributed to the presence of Si [148].
In conclusion, metal oxide nanotubes, particularly Ti dioxide nanotubes and their composites, show significant promise in enhancing bone regeneration through improved cellular interactions and functional properties, becoming suitable candidates for the advanced bone repair applications.
3.2.3
MOFs
When designing and synthesizing MOFs for tissue engineering, several critical factors must be considered. These include the structure and characteristics of the damaged tissues, the implementation of safe manufacturing methods, and the selection of appropriate metal ions, ligands, and functional groups to facilitate tissue regeneration (Fig. 5) [149,150].
Figure 5
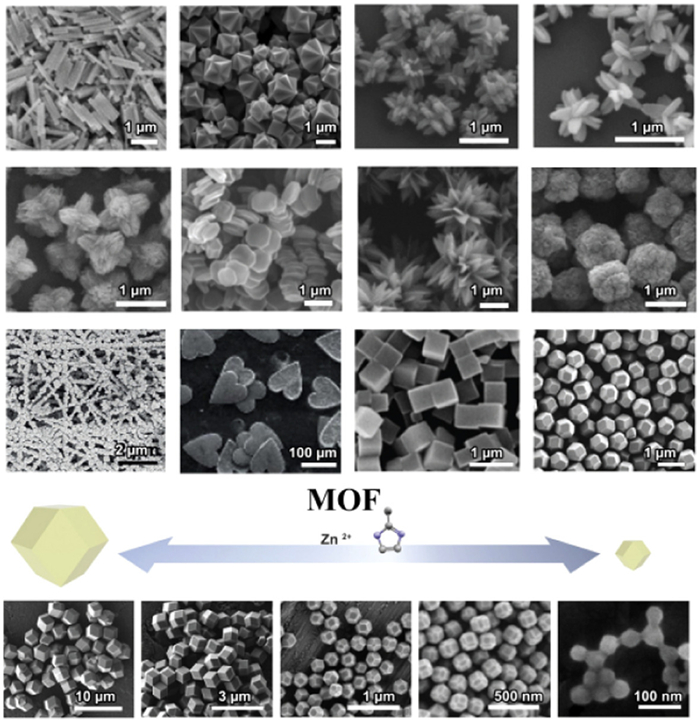
Figure 5.
Schematic diagram of the controlled morphology and size of MOF crystals. By changing the synthesis method, (adding metal ions) MOFs can be made into various shapes as needed. Reproduced with permission [150]. Copyright 2022, Elsevier.
Nanoscale MOFs possess unique properties such as high internal surface area, significant porosity, excellent thermal and chemical stability, mechanical robustness, biocompatibility, and tunability. Moreover, they can be easily recycled and reused [151]. Therefore, incorporating nanoscale MOFs into scaffolds is highly advantageous for the regeneration of damaged tissues.
Research indicates that modifying biomaterials with MOFs and nanoscale MOFs can alter the physicochemical properties of scaffolds, including surface roughness, functional groups, porous structure, and hydrophilicity. These changes are likely responsible for promoting cell adhesion and biological responses. Additionally, nanoscale MOFs can serve as carriers within polymer scaffolds to load essential growth factors for cell differentiation and antibiotics to prevent infections [149]. MOFs can enhance the mechanical properties of scaffolds designed for various types of bone defects, fractures, or atypical designs. The incorporation of specific drugs into these scaffolds can further aid in infection prevention, mitigate excessive immune responses during inflammation, and promote tissue regeneration. For instance, Lu et al. [152] constructed a Mg/Zn MOFs coating on alkali-treated Ti surfaces, demonstrating good stability and early anti-inflammatory properties on natural Ti substrates. The nanoscale structure and topological features of nanoscale MOFs enhance the physical and chemical properties of scaffolds, enabling effective drug loading, ion release, and the regulation of transplanted stem cells’ attachment, proliferation, and differentiation, thus broadening their applications in bone-related diseases and repairs. Liu et al. [153] incorporated Cu2+ into Mg-MOFs, highlighting the combined benefits of low-concentration Cu and Mg binding, which exhibited antibacterial, osteogenic, and angiogenic properties. This approach provides valuable insights for advancing the treatment of bone diseases. Similarly, Rojas et al. [154] introduced a Zn-based MOF that demonstrated high stability in phosphate-buffered solutions at pH 7.4 but significant degradation at lower pH levels. As a nano drug carrier, this metal ion MOF releases biomolecules and therapeutic agents in acidic environments, making it an attractive option for biomedical applications, drug delivery systems, and tissue engineering.
In summary, the integration of MOFs into composite scaffolds or coatings, along with the use of drug-targeting systems and advanced material technologies, represents a promising avenue for future research and progress in the field of MOFs.
4.
Application of metal-based biomaterials in different bone diseases
Bone is a dynamic tissue that undergoes continuous remodeling, characterized by highly regulated interactions between bone formation and resorption. This intricate process is crucial for lifelong bone repair and renewal, involving various biological mediators, including growth factors, cytokines, hormones, and regulatory signals. The balance of these mediators is vital for maintaining healthy bone structure and function [155]. However, disruptions in the activity of cells responsible for remodeling can lead to various bone-related diseases, including osteoporosis, bone dysfunction, osteosarcoma, OA, and metastatic bone cancer [156]. These conditions significantly affect the patients' quality of life and may even pose life-threatening risks. Although several treatment options utilizing advanced bioactive biomaterials are currently available, there remains a substantial need for innovative solutions capable of fully healing and restoring bone to its original state. In this context, metal-based biomaterials show promise as effective repair materials for bone tissue diseases. Comprehensive discussion regarding the application of metal-based materials in various bone diseases are provided in Supporting information (4.1–4.4, Figs. S2–S4).
5.
Conclusion and prospect
In recent decades, metal-based biomaterials have become essential in tackling the challenges related to the repair of bone diseases, their remarkable properties-such as promoting cell migration, inducing angiogenesis, upregulating osteogenic genes, and activating the immune system-have positioned them as critical components in the field of regenerative medicine. This article reviews various macroscale and microscale metal-based biomaterials employed to enhance bone integration and repair. Recent research has primarily concentrated on improving the biological activity of these metal materials through physical and chemical treatments, as well as utilizing composite forms to modify their surfaces. However, despite the superior mechanical properties of many metal materials, there is still a lack of comprehensive reports on safety, degradation behavior, corrosion resistance, stability of loading techniques, infection risk assessment, and rates of new bone formation associated with these materials. Furthermore, the physiological and pathological conditions of individual patients can impact the effectiveness of metal materials, underscoring the importance of personalized material selection and design. Lastly, cost considerations are also essential in the development and application of metal biomaterials. To better harness metal-based biomaterials for bone regeneration and repair, several challenges and issues must be addressed:
(ⅰ) Biocompatibility assurance: Ensuring the biocompatibility of metal-based materials intended for the repair of bone-related diseases is paramount. There is a need for the development of specialized nanostructures that enhance biological activity, alongside the construction of innovative composite metal biomaterials or microstructures using clinical animal models of bone defects. This approach will help ensure the long-term efficacy and stability of these materials.
(ⅱ) Targeted drug delivery: The repair of bone diseases within complex pathological microenvironments often entails addressing inflammation and damage to specific joints or tissues necessitates the development of drug delivery systems utilizing metal-based materials that can precisely target affected areas while minimizing off-target effects. Nonetheless, achieving efficient and selective drug delivery remains a challenge because of intricate anatomical structures and various physiological factors.
(ⅲ) Responsive therapeutic systems: Metal-based biomaterials intended for therapeutic applications should incorporate drug delivery mechanisms to construct responsive systems capable of intelligent stimulation. These systems can leverage multifunctional responses, including light, heat, magnetism, and electricity, while integrating biotechnologies such as 3D printing and electric field assistance, thus paving the way for enhanced bone disease repair.
(ⅳ) Scalable manufacturing processes: Optimizing morphological features and pore designs, ensuring appropriate chemical compositions, shapes, and sizes, and implementing effective surface modifications are crucial. Enhancements in wetting properties, biomimicry, adhesion, and bone immune regulation, along with the incorporation of bioactive ingredients, will facilitate improved bone disease repair.
In summary, the future of metal-based biomaterials in the context of bone disease repair is promising, with ongoing research focused on optimizing their properties and expanding their applications in clinical settings. Coping with the outlined challenges will be crucial in advancing the effectiveness and safety of these innovative materials in regenerative medicine.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
This work was supported by the National Natural Science Foundation of China (Nos. 52173150 and U22A20315), the Open Research Funds from the Sixth Affiliated Hospital of Guangzhou Medical University, and Guangzhou Science and Technology Program City-University Joint Funding Project (Nos. 2023A03J0001 and 2024A03J0604). Figs. 1 and 2 were drawn by using templates from Biorender. We sincerely acknowledge the funding and generous support from these foundations.
Supplementary materials
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.cclet.2025.111140.
S. Rojas, F.J. Carmona, C.R. Maldonado, et al., Inorg. Chem. 55 (2016) 2650–2663. doi: 10.1021/acs.inorgchem.6b00045
[155]
A. Wawrzyniak, K. Balawender, Animals 12 (2022) 1946. doi: 10.3390/ani12151946
[156]
A. Bagherifard, A. Hosseinzadeh, F. Koosha, et al., Osteoporosis Int. 34 (2023) 1677–1701. doi: 10.1007/s00198-023-06836-1
Figure 1
Classification diagram of metal-based biomaterials utilized for common bone-related diseases. The macroscale classification comprises metal alloys, Bioactive glasses, and bioceramic scaffolds. The microscale classification includes metal nanoparticles, metal nanotubes, and metal-organic frameworks.
Figure 2
Schematic diagram of biological effects of metal-based materials. (A) The functional regulation of osteoblasts and osteoclasts. (B) Modulating the inflammatory response to establish a supportive immune microenvironment for bone. (C) Upregulation of osteogenic genes and activation of signaling pathways. (D) Promoting angiogenesis in new bone formation. (E) Other biological effects (such as anti-tumor, antioxidant, and antibacterial).
Figure 3
(A) SEM images and photos of calcium sulfate based composite bioceramic bone cement: (a) Calcium sulfate, (b) 15% by weight mesoporous magnesium silicate, (c) 30% by weight mesoporous magnesium silicate, (d) photos of bone cement. (B) SEM images of bioceramic scaffolds on cell morphology: (a, b) 45S5 BG scaffold, (c, d) drug free chitosan PVP-45S5 Bioglass bone scaffold, and (e, f) vancomycin loaded chitosan/PVP-45S5 Bioglass bone scaffold. Reproduced with permission [77]. Copyright 2024, Elsevier.
Figure 4
(A) Schematic diagram of synthesis of single-crystal Co-MOF nanotubes. Reproduced with permission [144]. Copyright 2018, American Chemical Society. (B) Schematic illustration for the synthesis and structure of Co2+ doped single crystal MOF nanotubes. (C) The morphology and elemental mapping characteristics of Co-N/CNTs are presented: (a, b) SEM images depict the surface structure. (c–e) HRTEM images provide detailed insights into the internal features. (f) EDS elemental images illustrate the elemental distribution within the Co-N/CNTs. The illustration in (e) highlights the high-resolution lattice structure of CoNPs. Reproduced with permission [143]. Copyright 2021, Elsevier.
Figure 5
Schematic diagram of the controlled morphology and size of MOF crystals. By changing the synthesis method, (adding metal ions) MOFs can be made into various shapes as needed. Reproduced with permission [150]. Copyright 2022, Elsevier.

 DownLoad:
DownLoad:

 下载:
下载:






 下载:
下载:
