Citation:
Jingwen Wang, Peizhang Zhao, Mengmeng Li, Jun Li, Yunfeng Lin. Remedying infectious bone defects via 3D printing technology[J]. Chinese Chemical Letters,
2025, 36(9): 110686.
doi:
10.1016/j.cclet.2024.110686
Remedying infectious bone defects via 3D printing technology
English
Remedying infectious bone defects via 3D printing technology
Orthopedic Research Institute, Department of Orthopedics, West China Hospital, Sichuan University, Chengdu 610041, China
b.
Trauma Center, West China Hospital, Sichuan University, Chengdu 610041, China
c.
State Key Laboratory of Oral Diseases, National Center for Stomatology, National Clinical Research Center for Oral Diseases, West China Hospital of Stomatology, Sichuan University, Chengdu 610041, China
d.
Sichuan Provincial Engineering Research Center of Oral Biomaterials, Chengdu 610041, China
Received Date:
06 August 2024 Accepted Date:
26 November 2024 Revised Date:
20 November 2024 Available Online:
15 September 2025
Abstract:
The technology of three dimensional (3D) printing, also known as additive manufacturing, is a cutting-edge type of fabrication method that utilizes a computer-aided design platform and employs layer-by-layer stacking to construct objects with exceptional flexibility. Due to its capacity to produce a substantial quantity of products within a short period of time, 3D printing has emerged as one of the most significant manufacturing technology. Over the past two decades, remarkable advancements have been made in the application of 3D printing technology in the realm of bone tissue engineering. This review presents an innovative and systematic discussion on the potential application of 3D printing technology in bone tissue engineering, particularly in the treatment of infected bone defects. It comprehensively evaluates the materials utilized in 3D printing, highlights the interplay between cells and bone regeneration, and addresses and resolves challenges associated with current 3D printing technology. These challenges include material selection, fabrication of intricate 3D structures, integration of different cell types, streamlining design processes and material selection procedures, enhancing the clinical translational potential of 3D printing technology, and ultimately exploring future applications of four dimensional (4D) printing technology. The 3D printing technology has demonstrated significant potential in the synthesis of bone substitutes, offering consistent mechanical properties and ease of use. It has found extensive applications in personalized implant customization, prosthetic limb manufacturing, surgical tool production, tissue engineering, biological modeling, and cell diagnostics. Simultaneously, 3D bioprinting provides an effective solution to address the issue of organ donor shortage. However, challenges still exist in material selection, management of structural complexity, integration of different cell types, and construction of functionally mature tissues. With advancements in multi-material printing techniques as well as bioprinting and 4D printing technologies emerging on the horizon; 3D printing holds immense prospects for revolutionizing the means by which infectious bone defects are repaired.
The epidemiological data on infectious bone defects reveals that osteomyelitis poses a significant medical burden, with an approximate incidence rate of 22 cases per 100,000 individuals in the United States. Moreover, there has been a notable increase in its occurrence, particularly among the elderly population and those diagnosed with diabetes [1]. Infectious bone defects are typically caused by bacteria, with Staphylococcus aureus being the most prevalent and coagulase-negative Staphylococcus (CoNS) following closely behind [1]. Based on research, fracture-associated infection (FRI) is a potential complication following fracture treatment that places a significant burden on patients and healthcare systems alike. The incidence of FRI ranges from 2% for closed fractures to as high as 50% for open fractures [2]. Staphylococcus aureus is one of the most prevalent pathogens causing infectious bone defects, capable of forming biofilms to enhance its resistance. Moreover, it possesses inherent resistance to various antibiotics and can further evolve into methicillin-resistant Staphylococcus aureus (MRSA) through genetic mutations, thereby increasing the complexity of treatment. Coagulase-negative staphylococci, another common group of pathogens associated with medical device-related infections, exhibit resistance to multiple antibiotics, particularly methicillin-resistant strains, which complicates the management of infectious bone defects. Enterococci demonstrate resistance against a variety of antibiotics including vancomycin and linezolid; they may also cause infectious bone defects in certain cases. Additionally, Pseudomonas aeruginosa and Escherichia coli are frequent culprits behind infectious bone defects. These bacteria have shown an escalating trend in broad-spectrum antibiotic resistance, specifically producing multiple beta-lactam enzymes that can degrade beta-lactam antibiotics such as cephalosporins and penicillins [3].
Large areas of bone and cartilage injuries resulting from trauma, disease, or tumor removal mostly exceed the ability of bones to heal, and surgical repair and reconstruction are necessary [4]. Bacterial infections in bones can be caused by various factors such as trauma, surgical procedures, and the use of implants. In particular, implant-related infections in orthopedic surgery are prevalent. Effective infection control measures include the debridement of the infected area, systemic administration of antibiotics, and the use of antibiotic-impregnated spacers [5]. However, the efficacy of antimicrobial agents in infection prevention is compromised due to vascular destruction and osteonecrosis caused by infection. Additionally, poor penetration into bacteria biofilms poses a significant challenge, which exacerbates drug resistance of numerous pathogens, such as MRSA and multi-drug resistant Acinetobacter baumannii (MRAB), to antibiotics, thereby gravely threatening public health [6]. To address this issue, the idea of incorporating antimicrobials into implants has been proposed. Common clinical and surgical approaches used to repair bone defects include autologous/allogeneic bone and cartilage transplantation, vascularized bone transplantation, autologous chondrocyte implantation, mosaic plasty, and joint replacement [7]. The application of autologous transplantation is restricted by limited sources, while the problem of immune rejection facing allotransplantation limits its practicality [8].
Three dimensional (3D) bioprinting is a novel field of regenerative medicine that utilizes computer-controlled printers to precisely deposit bioinks containing living cells, biomaterials, and other biological substances in a layer-by-layer manner to create an optimal environment for simulating cell migration, proliferation, and differentiation of various tissues within the human body. It not only has high potential in tissue regeneration, but also plays an important role in drug delivery, cancer research and so on [9], and has become one of the most advanced tissue engineering methods [10]. 3D printing has become widely used in various medical domains such as personalized implant customization, prosthetics manufacturing, surgical tool fabrication, tissue engineering endeavors, biological modeling practices, and cell-based diagnostics, and the use of this technology to manufacture scaffold materials has become a new research hotspot. 3D bioprinting provides an effective solution to the limited capacity of organ donors by enabling the fabrication of diverse organ and tissue structures [11]. 3D printed scaffold materials boast a simple structure, high mechanical strength, and excellent biocompatibility. They can serve as a bone substitute and help repair bone defects. E. coli, methicillin-susceptible Staphylococcus aureus (MSSA), MRSA, and Pseudomonas aeruginosa were included to develop mature bacterial biofilms that could prevent postoperative bone infections [12].
The interaction of most bacterial enzymes and biosurfactants with a single extracellular polymeric substance (EPS) component threatens separation and stability, whereas the utilization of 3D bioprinting enables the production of robust and cost-effective synthetic dispersants capable of interacting with all three main EPS components [6]. The method shows promising potential as it opens novel avenues for research in the domains of medicine and biomaterials. With its remarkable versatility, 3D printing technology is widely used in the medical field and holds significant promise for further development. This review provides an in-depth exploration of the potential applications and advancements in 3D printing technology for infectious bone regeneration and repair. It delves into various aspects such as the materials utilized in 3D printing, the intricate processes involved in bone regeneration and repair, and the cells associated with this regenerative process. Despite its current nascent stage, this review emphasizes that there is immense promise for further development of 3D printing technology within biomedicine.
2.
3D printing materials
The bio-inks, one kind of fluid that can be easily extruded and rapidly solidified, serve as the foundational material for scaffold formation and retain their shape through physical or chemical stimulation [13]. The bio-inks can be loaded with bioactive molecules and cells with simple procedures to facilitate the adhesion, proliferation, and differentiation processes of target cells. However, it is challenging to find bio-inks that possess both the necessary physicochemical cues for cell biology and the required properties for 3D printing since these properties are often incompatible [14]. The design of bio-inks also requires a comprehensive understanding of the tissues and organs, which are composed of cells embedded in ECMs such as collagen, elastin, glycoproteins, proteoglycans, and growth factors [15], in order to meet both structural and functional needs. In recent years, the unique formulations of gelatin methacrylate (GelMA), collagen methacrylate, fibulin, and lamina-Ⅲ were finalized through comprehensive evaluation of the printable, active, adhesion, and other properties of bio-inks [16]. The utilization of bio-inks for creating implantable 3D hydrogel structures necessitates the incorporation of cell encapsulation capabilities as well as sufficient printability [17]. The primary challenge in the design of an optimal biodegradable bone replacement material lies in the precise control of degradation time, degradation behavior, mechanical properties, and processability of the implant material [18]. Following extensive research, 3D printing inks suitable for bone regeneration are primarily categorized into metallic, polymeric, ceramic and bioglass compositions, as well as 2D materials and other variants.
2.1
Metal
In metals and their alloys, the tradeoff between mutually exclusive properties such as yield strength and fracture toughness is unavoidable [19], since fracture resistance depends on lower yield strength and greater strain hardening [20]. Different metal materials exhibit varying favorable properties concerning bone regeneration, yet they also possess their own limitations. The key resolution lies in maximizing their advantages meanwhile mitigating their disadvantages. Specifically, titanium (Ti), cobalt-chrome-molybdenum, tantalum, magnesium, zinc, vanadium, strontium, gallium, barium, magnesium alloy, zinc alloy and other materials can be used as potential options for bone regeneration. Among them, Ti and Co-Cr-Mo alloys demonstrate commendable mechanical strength, mechanical property, biocompatibility and corrosion resistance, making them highly suitable for load-bearing implant design and cost-effective solutions [21]. Ti alloys are also often used as a reference to assess the capabilities of each additive metal in the manufacturing process [22]. However, the rate of osseointegration between the surface of Ti implants and new bone is considerably slow (Fig. 1A) [23], often resulting in delayed osseointegration or even insufficient integration and aseptic loosening [24]. Research has demonstrated that modifying the surface of Ti implants can enhance bone integration. Techniques such as sandblasting, acid etching, or coating the implant surface with bioactive molecules like hydroxyapatite have shown improvements in bone contact and accelerated integration process. These modifications promote attachment and growth of bone cells, thereby enhancing both speed and quality of bone integration. Furthermore, nanoscale modification of Ti surfaces has been proven effective in promoting osteoblast adhesion, proliferation, and differentiation. Compared to traditional smooth surfaces, nanostructured surfaces significantly improve the rate of bone integration.
Figure 1
Figure 1.
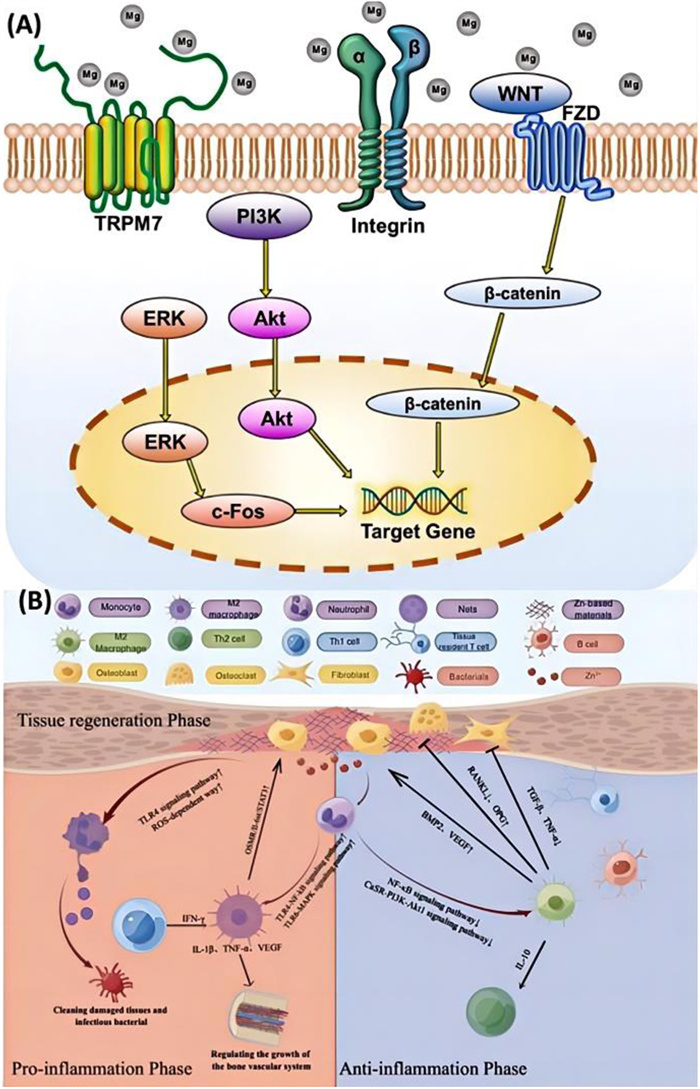
(A) Examples of mechanisms through which coatings containing magnesia enhance osseointegration in implants involve the activation of transient receptor potential melastatin 7 (TRPM7) protein channels and magnesium ions within integrin, extracellular signal-regulated kinase pathway (ERK), wingless-type (WNT) MMTV integration site family member, and PI3K pathways. Reproduced with permission [23]. Copyright 2023, Elsevier. (B) The immune response to treatment with zinc-based materials involves the initial recognition of pathogens by neutrophils and monocytes. Subsequently, M1 macrophages undergo polarization into M2 macrophages, which then mediate the expression of anti-inflammatory factors, thereby participating in adaptive immunity. Finally, during the tissue healing phase, M2 macrophages secrete relevant factors that promote wound healing and reconstruction. Reproduced with permission [25]. Copyright 2023, Elsevier.
Magnesium (Mg), the second most abundant cation in human cells, with over half of its content stored in bones, shows excellent biocompatibility, which renders magnesium alloys highly suitable as absorbable scaffolds. Amagnesium coating can enhance the bone density around the implant, facilitating its integration and healing within cancellous bone, and has antibacterial effect [25,26]. The presence of magnesium ions promotes cellular adhesion, propagation, osteogenesis, and angiogenesis via different pathways [26]. Thin films of bioactive magnesium hydroxide have been developed through hydrothermal treatment, and nanostructures capable of releasing magnesium ions have been discovered to enhance bone formation by activating signaling pathways associated with bone morphogenic protein-4 (BMP-4) mediated bone morphogenesis [27]. The activity of acid phosphatase (ALP) can be effectively improved, and zinc can also play an antibacterial role. Zinc-based biomaterials encompass metal zinc alloys, zinc-based ceramics, and zinc metal-organic frameworks (MOFs), which find extensive applications in tissue engineering due to their exceptional properties (Fig. 1B) [25]. In the process of natural wound healing, early recruitment and subsequent transformation of pro-inflammatory M1 macrophages into anti-inflammatory M2 macrophages occur [25]. The utilization of zinc-based material facilitates this transition of macrophages from M1 to M2 phenotype and enhances bone formation as well as wound healing [28]. The incorporation of strontium can also attenuate the immune response of the host to the material, thereby facilitating in-vitro bone regeneration [29]. Gallium based liquid metal (LM) is a metallic fluid at room temperature [30] with good fluidity, deformability, low melting point and strong self-healing ability [31]. The incorporation of LM into polymer materials has demonstrated the ability to exhibit shape memory properties under thermal or electric stimuli [32]. The fluid properties of LM simultaneously prevent excessive changes in mechanical properties and enable the shape of LM to be altered within the polymer matrix, thereby enhancing its capacity for shape recovery [33]. Moreover, the crosslinking capacity and impact of barium have been widely acknowledged as superior to other metal cations, which can enhance the mechanical stability of the structure and therefore resulting in better bone defect repairs with elevated mechanical properties. Furthermore, during the later stages of implantation, the formation of a corrosion product layer further enhances its osteogenic capability [34]. The low melting point and chemical inactivity of Zn can effectively inhibit osteoclast-mediated bone resorption and promote osteoblast-driven bone formation, thereby enhancing bone mass. Additionally, Zn ions possess the ability to disrupt bacterial cell membrane integrity and induce protein degeneration within cells, thus exhibiting fungicidal properties [35]. Biodegradable zinc alloy, as another novel biodegradable metal material with a moderate degradation rate and excellent mechanical properties, is also considered to possess the potential to serve as an ideal scaffold for bone tissue engineering [36]. By incorporating magnesium into the zinc alloy, not only does it possess tissue-filling capabilities but also demonstrates osteogenic effects [37]. Compared to Ca-Zn, Li-Zn, and Fe-Zn alloy scaffolds, Zn-Mg alloy scaffolds ensure the mechanical strength of the scaffolds while maintaining excellent biocompatibility and bone healing ability. Simultaneously, the porous zinc metal scaffold gradually degrades and is reabsorbed during the bone defect healing process, achieving autogenous bone repair effectively. This has significant clinical implications for patients' rehabilitation from bone defects [38]. Silver has antibacterial properties, is effective against bacteria by adsorbing bacterial proteases, can improve mechanical properties and maintain the biocompatibility of silver-containing materials. Therefore, the addition of magnesium and silver to zinc alloys may enhance osteogenic and antimicrobial properties while ensuring biocompatibility, excellent mechanical properties and biodegradability [39]. The Zn-2Ag-0.04Mg alloy exhibits excellent biocompatibility and bone induction efficiency, along with potent antibacterial activity against Staphylococcus aureus and Staphylococcus epidermidis. Furthermore, it demonstrates controlled degradation kinetics and significantly enhances in vivo bone regeneration, as previously validated in scientific investigations [40].
2.2
High-molecular polymer
The polymer exhibits distinctive characteristics in terms of its mechanical properties, stability, and biocompatibility [41]. The classification primarily consists of two categories: natural polymers and synthetic polymers. Synthetic polymers are biocompatible materials that, upon the addition of bioactive ingredients, can effectively mimic the properties of natural extracellular matrix (ECM) [42]. The following outlines the distinctive features of each. A detailed description of polymer materials can be seen in Supporting information.
2.3
Ceramics and glass
Bioactive glass and glass-ceramics are also widely utilized as bone tissue regeneration materials due to their ability to enhance osteoblast adhesion, promote differentiation of MSCs and progenitor cells, as well as facilitate angiogenesis [21]. The material known as bioactive glass is composed of a crystalline phase embedded within an amorphous glass matrix, while microcrystalline glass belongs to a class of materials that lies between traditional glass and polycrystalline ceramics, exhibiting distinct biological and mechanical properties compared to the parent glass [21]. The glass-ceramics exhibit excellent biocompatibility, exceptional chemical durability, outstanding wear resistance, remarkable fracture strength and toughness, as well as low thermal conductivity. The mechanical strength of lithium disilicate (LD) glass-ceramics is enhanced by the incorporation of nuclear agents such as P2O5, Ti2, ZrO2, and Nb2O5. Additionally, the inclusion of K2O, Al2O3 and CeO2 improves the chemical durability, densification, and mechanical properties of LD glass-ceramics. The material of quartz glass exhibits exceptional optical transparency, as well as remarkable thermal, chemical, and mechanical resilience, rendering it indispensable in contemporary engineering applications. Nevertheless, its structural modification poses challenges due to its softening point reaching up to 1100 ℃ [43]. The realization of 3D free-form surface manufacturing of silica primarily depends on the utilization of particle-loaded adhesives and sintering technology [44]. Ceramics possess exceptional mechanical properties, including structural stability [45], wear resistance [46], corrosion resistance, and high temperature resistance [47]. Consequently, they are widely employed in biomedical fields such as bone tissue engineering and hard tissue regeneration. The brittleness and hardness of ceramics pose challenges in the manufacturing of intricate ceramic supports using conventional molding processes, which can impede precision and efficiency [48]. The utilization of additive manufacturing technology enables the production of intricate ceramics with integrated structure and functionality, enhancing their flexibility and consequently propelling the advancement in high-performance ceramic materials [49]. Direct ink writing (DIW), an extrusion-based additive manufacturing technique commonly employed at mesoscale and microscopic scales, can be combined with photoassisted photopolymerization to fabricate ceramic scaffolds that exhibit exceptional strength and functionality [50]. The near-infrared radiation (NIR)-assisted DIW technology simultaneously enables the simulation of intricate structural levels found in real bone tissue, thereby accurately concentrating micro- and nano-scale characteristics within the ceramic scaffold [51]. Consequently, this enhances the scaffold's capacity to facilitate cellular attachment, proliferation, and differentiation [52]. Moreover, the incorporation of bioactive components into 3D printed ceramic structures and the integration of growth factors, drugs or signaling molecules during printing can facilitate tissue regeneration [53], angiogenesis [54], immune modulation [55], and enhance the therapeutic efficacy of implants for bone repair and regeneration.
2.4
Black phosphorus (BP)
The emerging nanomaterial, BP, possesses a unique structure and stability, along with exceptional mechanical properties, electrical conductivity, thermoelectric properties, biocompatibility and biodegradability, making it highly promising for applications in the biomedical field. The degradation of BP in the human body through reaction with water and oxygen results in the formation of non-toxic phosphonates and phosphates. It is worth noting that phosphorus, a crucial element for bone formation, exists abundantly within the human body [56]. Therefore, BP is a commonly used 3D printing material for bone regeneration. However, its practical applications are limited due to its low stability caused by easy reaction with water and oxygen under various environmental conditions. To address this issue, surface functionalization is often conducted through physical or chemical modifications to effectively isolate BP from oxygen and water, thereby ensuring its original physical and chemical properties [57]. The cytotoxicity of BP was found to be lower than that of graphene but higher than transition metal dihalides, with toxicity positively correlated with concentration, size, and thickness [58]. Unmodified BP exhibited significant cytotoxicity. In-vivo experiments demonstrated that the majority of administered BP is excreted through feces and urine without causing substantial damage to vital organs [59]. Therefore, further exploration and optimization of BP parameters are necessary to ensure its safety in biomedical applications.
2.5
Smart materials
The classification of a substance as "intelligent" is attributed to its remarkable capacity to perceive and adapt to changes in its environment, hence why these components are commonly referred to as "responsive materials". Smart materials encompass a diverse range of substances, including intelligent antimicrobial peptides, pit and crack sealants, impression materials, cement, and sutures. These materials exhibit altered properties in response to specific stimuli such as temperature variations, mechanical stress, humidity levels, pH changes, or electric and magnetic fields [60]. The recent focus in the field of bone therapy and regeneration has been on smart hydrogels that exhibit spatially and time-controlled responses to both internal and external stimuli [61]. The smart hydrogels, in comparison to conventional hydrogels, possess the capability to achieve adjustable, programmable, and controllable alterations as per demand for regulating the bone microenvironment [62] and exhibiting diagnostic and therapeutic functionalities in treating pathological bone defects [63]. In addition to providing structural support, smart hydrogels implanted into bone defects stimulate osteogenic and immune-related signaling pathways that regulate various cellular behaviors in the bone microenvironment, thereby facilitating bone regeneration [64]. Smart hydrogels offer significant advantages over traditional hydrogels in biological applications. They possess the ability to control the phase transition process between solution and gel state through their sensitive components [65]. Upon injection, heat-sensitive hydrogels can automatically transform from a solution into a gel state due to temperature increase. Following implantation, smart hydrogels can alter their chemical and physical properties in response to stimuli, thereby regulating cell activity within the microenvironment. Moreover, utilizing smart hydrogels for drug delivery reduces dosage frequency while maintaining therapeutic concentration levels required, thus minimizing drug accumulation in non-target tissues and mitigating potential side effects [65]. As research progresses on understanding the underlying mechanisms of bone-related diseases, future therapies targeting microenvironmental changes will be developed. Consequently, smart hydrogels that elicit distinct reactions within the bone microenvironment hold promising prospects for both research and market applications [65]. In addition, for a more detailed understanding of the commonalities and specificities between materials (Table S1 in Supporting information).
3.
Cells associated with bone regeneration
Bones possess inherent homeostatic abilities, but when faced with overwhelming damage such as severe trauma, malignant tumors, or infections, their capacity for self-regulation is limited. Consequently, the re-established equilibrium of bones becomes disrupted and therefore triggering a cascade of detrimental effects. The significance of non-coding RNA (ncRNA), specifically long non-coding RNA (lncRNA)/microRNA (miRNA) networks, in the progression of injuries should not be disregarded [66]. 3D printing technology enables the fabrication of tissue-engineered scaffolds that provide a conducive environment for seed cells to proliferate, allowing them to grow within the scaffold and gradually mature into living tissue. Simultaneously, it allows precise control over the multi-scale structure of bone tissue engineering scaffolds, which is crucial for mimicking the ECM and promoting bone regeneration. By accurately manipulating pore geometry, size, porosity, etc., it becomes possible to regulate the release of cytodynamics and bioactive factors [67]. The 3D printed scaffolds possess the ability to generate tailored or regulated therapeutic effects based on external and internal stimuli. These scaffolds induce MSCs to differentiate into osteocytes [67]. The utilization of 3D bioprinting facilitates the rapid generation of functional vascularized tissue within the construct, which is crucial for effective restoration of extensive bone defects. GelMA/gellan gum methacrylate (GGMA) bio-inks have exhibited exceptional printability and enhanced mechanical properties through dual cross-linking, thereby significantly promoting migration and formation of endothelial cells [68]. Moreover, it can enhance the endogenous bone regeneration process and achieve the dual function of overall cartilage and bone repair through the utilization of multicellular distribution and cell-induced bio-inks containing bioceramic particles. This 3D bioprinted co-culture scaffold has demonstrated its capability to induce osteogenesis and cartilage differentiation in vitro, as well as accelerate the repair of severe osteochondral defects in vivo [69]. Cells play an indispensable role in bioprinted tissue by influencing its biological properties; hence, the selection of cell type and source assumes paramount importance [15]. The excellent self-renewal and differentiation capabilities of stem cells have prompted their application in the field of bone tissue regeneration. Currently, MSCs, induced pluripotent stem cells (iPSCs), and embryonic stem cells (ESCs) are extensively utilized with remarkable success.
3.1
MSCs
The MSCs are pluripotent cells capable of self-renewal and differentiation into multiple cell types. They are widely distributed in human body, possess excellent proliferative potential, can be isolated from adult mesenchymal tissue [4]. MSCs can retain their multidirectional differentiation ability across multiple generations without any loss, and thus represent an ideal cell source for bone regeneration [70]. The chondrogenic potential of MSCs derived from synovium and subpatellar fat pad has been demonstrated to be superior to that of MSCs obtained from other tissues. MSCs possess the ability to undergo multi-directional differentiation, regulate immune responses and inflammation, as well as enhance angiogenesis, cell viability, and differentiation [71]. The activation, proliferation, maturation, cytokine production, cytolytic activity, and antibody production of innate and adaptive immune cells can all be intervened with MSCs. Additionally, these stem cells can also release anti-inflammatory cytokines to induce appropriate macrophage polarization and regulate inflammation [72]. The immunosuppressive effect is associated with the inhibition of T cell proliferation and the induction of regulatory T cells. Besides, MSCs can facilitate the polarization of macrophages from the anti-inflammatory M1 phenotype to the pro-inflammatory M2 phenotype and therefore promoting immune homeostasis [73]. The bone regeneration potential of MSCs in bone marrow, adipose tissue, periosteum, and muscle has been extensively investigated thus far [74]. The aforementioned evidence has demonstrated the practicality of MSC implementation in bone defect reparation, 3D printing, OA, and other related fields. However, it is also important to acknowledge the tumorigenic potential of MSCs as well as the immune rejection associated with allogeneic cells [75]. MSCs have demonstrated a remarkable efficacy in the repair of infected bone defects. MSCs exert immunomodulatory and anti-inflammatory effects through the secretion of various mediators, including cytokines and growth factors. These mediators possess the ability to attenuate the body's inflammatory response and facilitate tissue regeneration. Simultaneously, MSCs also promote neovascularization, exhibit antioxidant properties, inhibit apoptosis, and further enhance bone healing [76]. The Masquelet technique, when combined with BMSCs, has been employed for the treatment of infected bone defects, yielding favorable outcomes [77]. The studies have demonstrated that hypoxic preconditioning can significantly enhance the secretion and functionality of extracellular vesicles (EVs) in MSCs. When combined with bioactive hydrogels, it can effectively facilitate the formation and differentiation of skull osteoblasts, thereby achieving bone regeneration [76].
3.2
iPSCs/ESCs
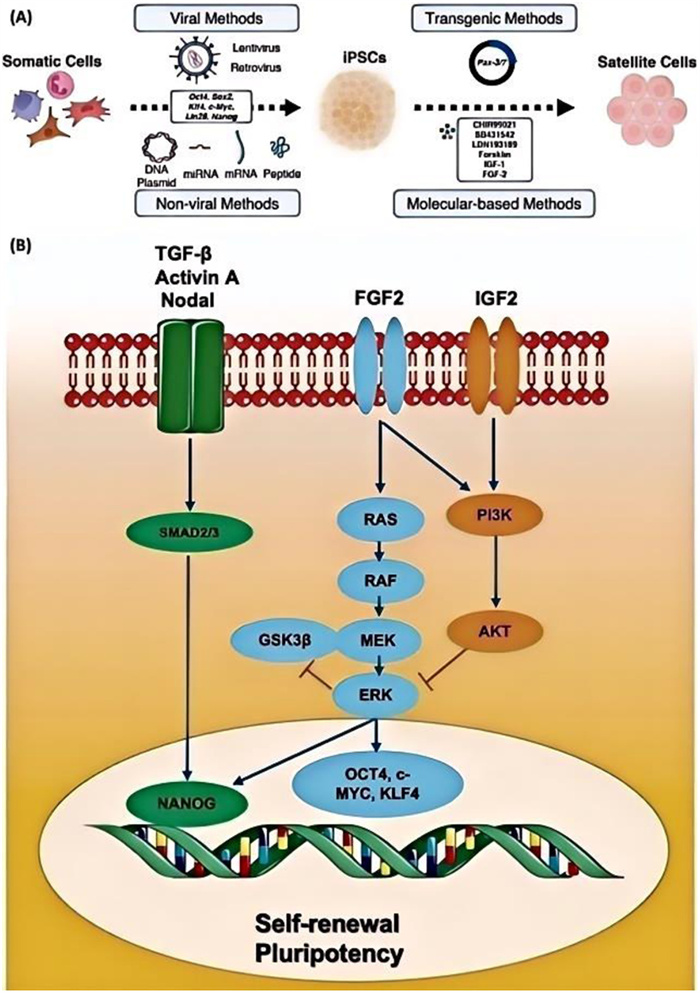
MSCs and chondrocytes can be induced to differentiate from embryonic stem cells [78]. The generation of iPSCs involves factor-mediated reprogramming of somatic cells, resulting in the acquisition of self-renewal capacity, pluripotency, robust proliferation, and efficient differentiation ability [21]. The above cells not only possess multiple tissue sources, but also demonstrate symmetrical division, leading to a substantial number of duplications with pluripotent properties. Furthermore, it exhibits the ability to differentiate into various cell types within the body, including neurons, cardiovascular and hematopoietic lineages, cardiomyocytes, and myogenic precursors. The reprogramming of somatic cells into iPSCs is achieved through the delivery of key transcription factors, including Oct4, Sox2, Klf4, and c-Myc, utilizing techniques such as retroviral vectors, lentiviral vectors, and non-viral approaches. Prominent methods include transgenic techniques and molecular-based approaches (Fig. 2A) [79]. The hypertrophic chondrocytes derived from iPSCs can undergo transformation into osteoblasts and bone cells both in vivo and in vitro [80]. The successful generation of human iPSCs and their differentiated derivatives has led to an increasing utilization in the fields of transplantation medicine, disease modeling, drug discovery, and personalized therapeutics [81]. Typically, human ESCs are cultured on mouse embryonic fibroblasts or without a feeder layer. For example, culture on matrigel in a medium containing basic fibroblast growth factor (bFGF) and activin A or TGF-β. bFGF signal transduction supports pluripotent, dry, and hESC self-renewal by activating the phosphatidylinositol 3-kinase (PI3K)/AKT pathway, inhibiting ERK activity, WNT signal transduction, and dephosphorylation of glycogen synthase kinase-3 (GSK3β) (Fig. 2B) [82]. The embryonic stem cells are derived from the inner cell mass of the blastocyst and possess an unlimited capacity for proliferation and pluripotency, which is meticulously regulated by precise external and internal networks encompassing epigenetic modifications, transcription factors, signaling pathways, and histone modifications. The co-culture system was confirmed to be capable of forming cell colonies and secreting ECM containing glycosaminoglycans, as evidenced by gene expression analysis and immunostaining [83]. The dynamic expression of chondrocyte-specific genes was observed during the diffusion of monolayer cells in this co-culture system, thereby confirming the chondrogenic differentiation of human embryonic stem cells [84]. Self-promoting electroactive mineralized scaffolds (sp-EMS) generate a weak current through spontaneous electrochemical reactions, activating voltage-gated Ca2+ channels, enhancing adenosine-induced actin remodeling, and ultimately facilitating osteogenic differentiation of MSCs. Simultaneously, the electroactive interface provided by sp-EMS inhibits bacterial adhesion and activity, leading to complete or near-complete in-situ healing of infected bone in vivo [85]. The main cause of death for BMSCs in the infected bone microenvironment is iron-induced cell death. Intervening in this process can partially mitigate cellular damage and restore osteogenic function. Building upon this discovery, a hydrogel composite 3D printed scaffold was designed to release antibacterial ammonium chitosan in response to ROS, while continuously delivering ferrostatin-1 (Fer-1), an inhibitor of iron-induced cell death. This innovative approach effectively eliminates pathogens and promotes bone regeneration in a rat model of infectious bone defect [86].
Figure 2
Figure 2.
(A) Methods and pathways of iPSC generation and further differentiation into satellite cells. Reproduced with permission [79]. Copyright 2023, MDPI. (B) Major signaling pathways regulating self-renewal and pluripotency of human embryonic stem cells. Reproduced with permission [82]. Copyright 2023, MDPI.
New advancements in the medical field of 3D printing technology and bone regeneration materials encompass the progress of bioprinting, utilization of smart scaffolds, and reconstruction of bionic structures and functions. These developments exhibit significant potential in enhancing treatment efficiency and promoting tissue regeneration. The technology of biological 3D printing integrates living cells and biological materials to precisely fabricate and implant tissues and organs in a layer-by-layer manner, enabling the precise arrangement of cells and biological materials in three-dimensional space [87]. This technique has emerged as a promising approach in the fields of bone tissue engineering and regenerative medicine [88]. The field of 3D bioprinting not only necessitates the simulation of tissue structure and mechanical properties, but also demands the reconstruction of its functionality. Its potential application in organ reconstruction presents a novel concept for the development of artificial organs and their clinical implementation. Despite yielding encouraging outcomes, 3D bioprinting still encounters certain challenges such as generating effective blood vessel networks to enhance tissue vitality [88]. Smart stents can produce customized or controllable therapeutic effects based on exogenous or endogenous stimuli. For example, Zhu and Han et al. pointed out that, compared with inert and functional bone grafts, next-generation smart stents have an extraordinary ability to simulate the dynamic properties of the natural ECM, thereby promoting bone repair and regeneration. It can respond to exogenous stimuli such as light, mechanical force, magnetic and ultrasonic stimulation, as well as endogenous stimuli such as body temperature, weakly acidic environment under special pathological environment, and inflammatory factors [67]. These stimulus-response strategies enable smart stents to maximize therapeutic effectiveness in a precisely controlled, efficient, and safe manner. The utilization of 3D printing technology offers significant advantages in personalized treatment, as it enables the precise fabrication of stents with appropriate dimensions, morphology, and inherent structural characteristics based on computerized axial tomography or magnetic resonance imaging scans of individual patients. This tailored approach to treatment can effectively address specific patient requirements and enhance the efficacy and success rate of interventions [89]. Emerging techniques in bone tissue engineering have made remarkable progress in advancing the treatment of bone defects. However, there are still several challenges that need to be addressed, including material fatigue, enhanced biological activity, and the realization of more complex tissue structure bionics. Currently, widely used 3D printing materials have certain limitations in terms of durability and fatigue resistance. Therefore, it is necessary to strengthen research and development efforts towards new materials such as higher performance metal alloys and composite materials to improve their mechanical properties and stability. Furthermore, by enhancing the 3D printing process through adjustments in printing parameters and post-processing procedures, it is possible to effectively reduce stress concentration within the material and enhance the fatigue resistance of the final product. In order to promote biological activity within bone tissue engineering, it is crucial to develop biocompatible and bioactive materials that facilitate cell growth and tissue regeneration inside the human body. Simultaneously, studying methods for maintaining cell viability during the printing process becomes essential. This includes synthesizing bioinks capable of mimicking natural ECM while improving mechanisms for loading and releasing cells. Additionally, developing mild bioprinting technologies like low-temperature printing or light-curing technology can help minimize pressure on cells during construction processes. These advancements enable cells to remain active within more complex biological environments while facilitating precise arrangement and structural construction of various cell types. In order to achieve optimal outcomes, stents should be thoroughly tested as part of a comprehensive tissue regeneration regimen, combined with novel techniques for managing soft tissues. Enhancing scaffold design and developing advanced biomaterials such as degradable polymers are crucial areas for future research. Additionally, 3D printed scaffolds hold great promise in the field of bone tissue engineering [90]. Compared to conventional manufacturing technologies, 3D printing technology offers the advantages of enhanced automation, superior precision, and a wide array of material options. Moreover, it possesses the capability to efficiently and accurately pattern cells, growth factors, and biological materials in order to construct intricate 3D tissue structures [91]. Therefore, it enables a wide range of potential applications in the field of biomedicine. The excellent corrosion resistance and high tensile strength of porous titanium alloys make them extensively utilized in orthopedic applications, such as intramedullary nails (Fig. 3A) [92]. The integration of 3D printing technology and biomedicine represents one of the most significant future directions of medical science, as it can compensate for the limitations associated with traditional medical device manufacturing techniques, thereby enhancing efficiency meanwhile reducing costs in medical device production, ultimately leading to great leaps within the healthcare industry. Simultaneously, 3D printing holds significant promise in promoting bone regeneration and repair by enabling bone transplantation procedures that can mitigate the adverse effects brought by immune rejection, disparate density levels, and inadequate biochemical functionality [21]. However, 3D printing technology is still at its early stages, and there are numerous challenges that need to be addressed.
Figure 3
Figure 3.
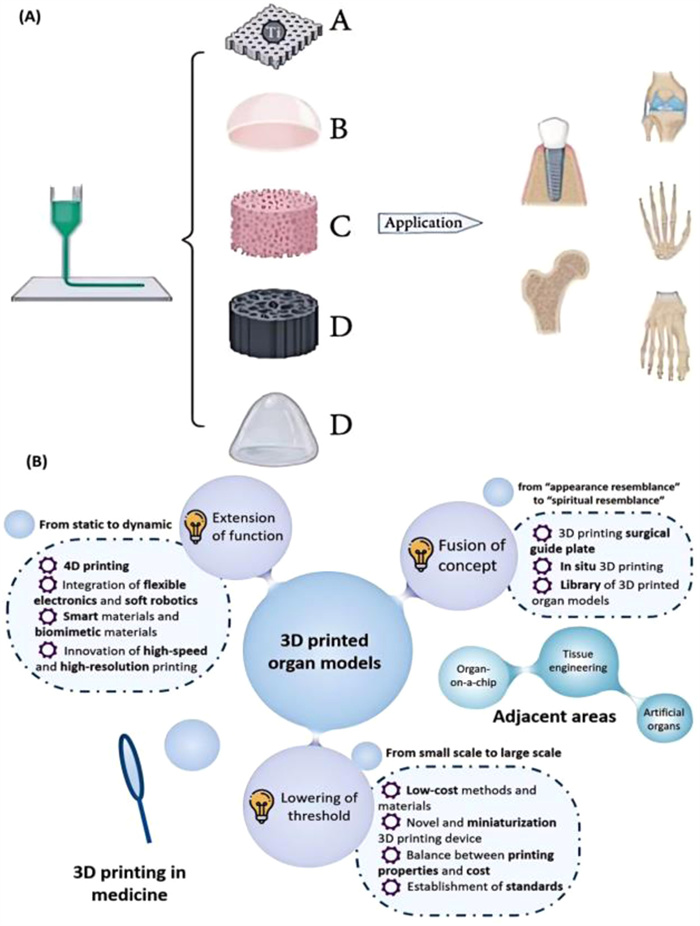
(A) The utilization of additive manufacturing technology in the field of orthopedics. Reproduced with permission [92]. Copyright2022, Hindawi. (B) Future development of organ model 3D printing. Reproduced with permission [93]. Copyright 2021, Wiley.
First, material selection is of great importance in determining the performance of 3D printed products. Different materials exhibit varying levels of biocompatibility, biodegradation rate, and mechanical properties; therefore, careful consideration should be given to selecting appropriate materials for bone repair applications. Secondly, for products with intricate three-dimensional structures and high precision requirements, advanced techniques such as multi-layer printing or composite printing should be employed. Thirdly, 3D bioprinting encounters the obstacles of integrating diverse cell types, constructing multi-scale vascular systems, and achieving functional maturity equivalent to adult tissue [15]. Besides, it holds significant importance in the production and manufacturing of products that have urgent clinical requirements, small product sizes, simple structures, and short manufacturing cycles. Therefore, there is a need to simplify the design process and material selection procedures for 3D printing technology. Also, the need for further development in the clinical translational aspects, such as large-scale cell production and differentiation, bioreactor platforms for post-printing tissue maturation culture, and the establishment of comprehensive regulatory pathways for organ-scale construction is urgent [15]. On the other hand, 3D bioprinting holds immense potential in the realm of cancer research and treatment by accurately replicating the tumor microenvironment, facilitating drug efficacy testing, and enabling the construction of intricate physiological structures. Nevertheless, challenges persist in terms of resolution limitations and the absence of vascular networks. Fortunately, these obstacles can potentially be overcome through a synergistic integration of innovative technologies. The current trend in 3D printing is moving towards multi-material printing, bioprinting, and four dimensional (4D) printing. With the continuous innovation of the technology and materials for 3D printing organ models, various new methods not only gradually meet the growing demand, but also break through the existing limitations of organ models (Fig. 3B) [93]. Simultaneously, advancements in smart composites, soft robotics, and flexible electronics are revolutionizing the operational landscape of the industry. Particularly, photopolymerization exhibits remarkable potential in areas such as tomography printing, 3D nanocrinting, and the manufacturing of superhydrophobic objects. Furthermore, additive manufacturing and its associated materials can also be effectively applied to water resources treatment, medical fabrication, and various other fields. It is anticipated that these strategies will pave the way for addressing cancer-related concerns in future endeavors.
5.
3D printing for the repair of infected bone defects
3D bioprinting enables the customizable fabrication of biological materials based on digital design and facilitates the creation of precise geometrical structures [14]. The key technologies encompass fused deposition modeling (FDM), extrusion-based 3D bioprinting (EBB), selective laser sintering (SLS), direct ink writing (DIW), stereolithography (SLA), and so on [94]. The process of melt deposition modeling involves melting a thermoplastic polymer into a semi-liquid state and extruding it onto a build platform, which is considered as one of the conventional techniques. By depositing the material layer by layer, a solid geometry can be formed, thereby improving parameters such as Young's modulus, tensile strength, processing temperature, and density [94]. A coating production material was then developed that uses laser cutting and welding to connect each layer. The technology equipment exhibits a low cost of raw materials, high utilization rate, and an extensive selection range [95]; however, it demonstrates limited precision in constructing complex structural components, low perpendicular section strength, and slow molding speed [96]. The aforementioned statement describes a cutting-edge and extensively utilized 3D printing technology renowned for its accessibility, versatility, and applicability across diverse industries. Extrusion-based 3D printing technology features a straightforward printing process and cost-effective manufacturing, but necessitates meticulous consideration of material quality and printing parameters due to the significant influence of ink's viscoelasticity, inorganic impurities, and processability on extrusion efficiency and printed structure quality [94]. The technology can effectively promote cellular activity and facilitate the regeneration of functional tissues, making it extensively applied in the biofabrication of skin, bone, and myocardium. Selective laser sintering involves the melting of metal and non-metal powders by melting a binder or a metal with a low melting point, that is, ceramic powders and other low-melting powders are laid on a powder bed, and the laser is programmed to move in accordance with a set path, so that the low-melting powder melts and connects the ceramic particles under the influence of the laser [97]. The unique feature of SLS technology is that it eliminates the need for a support structure, as the printed part is supported by the powder itself [98]. The degradation of used powders at high temperatures may necessitate future printing for new materials. However, the ability of SLS to reuse materials in subsequent operations establishes it as an environmentally friendly production technology with minimal labor requirements and consistent results across multiple batches [99]. SLS molding process exhibits high speed, a wide range of molding sizes, however, it is characterized by a relatively high organic adhesive content resulting in low object density with loose and porous structures. To address this issue, the density can be increased through isostatic pressure treatment or penetration technology [100]. The selective laser sintering technology finds diverse applications in the field of medical engineering, encompassing the fabrication of surgical physical models, prototypes for medical devices, and scaffolds for tissue engineering. SLS 3D printers are widely favored in product development owing to their cost-effectiveness, high productivity, and material versatility. They have the capability to produce a wide range of materials including plastics, metals, glass, ceramics, and composites [98]. DIW refers to the process of uniformly dispersing ceramic powder and blending it with various organic compounds to create a ceramic ink [101] that possesses appropriate viscosity, surface tension, electrical conductivity, and drying rate. This ink is then printed onto a flat surface to produce ceramic blanks, which are subsequently degreased and sintered in a high-temperature furnace [102]. The fast formation speed and versatility in raw material usage make it advantageous for the production of dark ceramic products [96]. It is primarily employed for printing modern construction sites and other large-scale objects. In contrast to the FDM process, DIW does not require high-temperature slurry melting. Instead, it is extruded through a nozzle at ambient temperature and solidifies on the structure's surface. Furthermore, various types of slurry can be manipulated using multi-nozzle coordination or a single nozzle, enabling the fabrication of functionally adjustable gradient structures [103]. The dominant, versatile, and widely recognized 3D printing technique for producing photosensitive ceramic pastes involves the combination of ceramic powders, photosensitive resins, and other additives through SLA [104]. The technique employs a powerful ultraviolet laser to initiate a reaction that gradually solidifies the liquid resin layer by layer, precisely guiding the laser onto the resin through a detachable mirror galvanometer which directs the beam to an exact location. The polymerization is intentionally left incomplete during the printing process and subsequently finalized post-printing in order to enhance cohesion between consecutive layers [105]. The SLA process is frequently employed for the production of small parts with intricate shapes, owing to its notable advantages in terms of rapid formation, excellent surface quality, and high dimensional accuracy [96]. Overall, FDM offers a cost-effective solution in terms of equipment, materials, operation and maintenance, making it one of the most economical 3D printing technologies available. Despite the initial investment and maintenance costs associated with extrusion-based 3D bioprinting, its application value remains unparalleled in the field of personalized medicine and biomedicine, promising substantial long-term returns on investment. SLS and DIW may be relatively expensive options; however, they excel in producing high-quality and intricate products suitable for advanced manufacturing and precision printing applications. SLA proves to be a cost-effective choice for prototyping and small batch production needs while particularly excelling in complex geometry modeling. The selection of bioinks and the level of structural complexity achievable in bioprinting are determined by different printing technologies [42]. The application of 3D printing technology in orthopedic surgeries greatly enables the manufacturing and repair of joints, spine, skull, lower limb bones, etc. [106]. A 3D printed model was used for fracture reduction and a customized personalized plate was used for fixation (Fig. 4A) [107]. This advanced method outperforms traditional manufacturing techniques by using different materials to produce complex bone structures efficiently, in terms of both time and costs. Moreover, it addresses concerns regarding tissue sources, immune rejection, disease transmission, and virus contamination while enhancing biocompatibility. The reconstruction of a normal bone structure, including both dense and spongy bone, requires the use of bone scaffolds, cells, and growth factors [108]. Additionally, 3D bioprinting enables the deposition of living cells and biomaterials.
Figure 4
Figure 4.
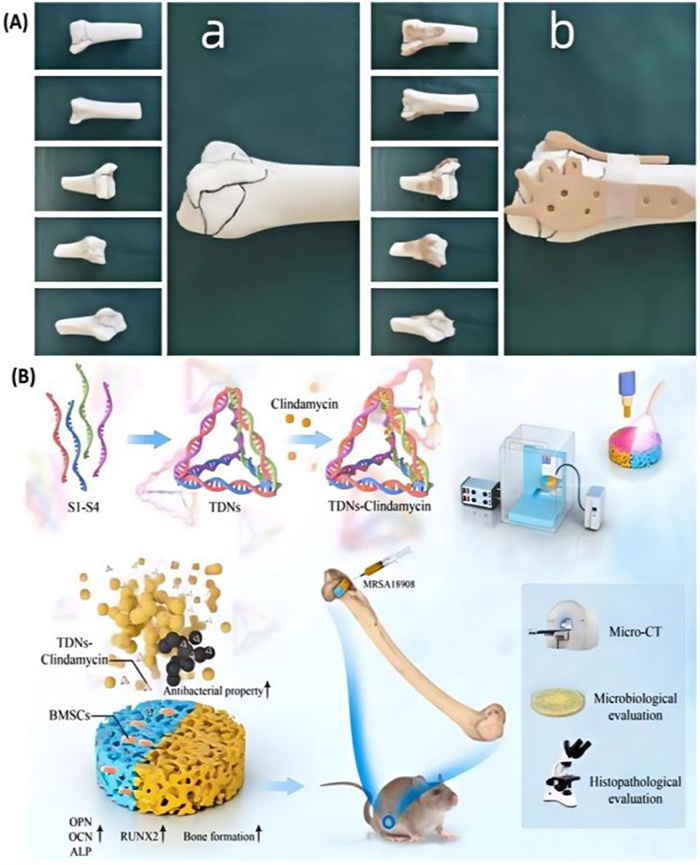
3D bioprinting allows efficient production of complex bone structures. (A) 3D printed model after virtual fracture reduction. Appropriately customized plates and fracture 3D models are sterilized and on standby for use during surgery [107]. Copyright 2023, Nature. (B) The synthesis of TDN—CLI complex and the construction of TDN—CLI supported 3D bioprinting composite scaffold, show excellent antibacterial and osteogenic properties. Reproduced with permission [106]. Copyright 2022, Elsevier.
With the continuous advancement and evolution of 3D bioprinting technology, numerous practical instances have emerged where it has been successfully employed for the regeneration of extensive bone defects. In a clinical trial conducted by Lee et al. [109], CaoSiO2-P2O5-B2O3 glass-ceramics (BGS-7) were utilized as an implant to address cheekbone defects. Computerized tomography (CT) observations revealed complete bone fusion after a period of 6 months, exhibiting no indications of osteolysis, while the displacement of the implant measured approximately 0.4149 mm post-treatment duration. This study demonstrated remarkable efficacy in promoting cheekbone healing with a satisfaction score rating at 9 [110]. Faldini et al. [111] utilized cobalt-chromium-molybdenum powder and polyamide to tailor a high-strength metal ankle implant for a 57-year-old male patient. Four months post-surgery, the clinical score demonstrated highly satisfactory outcomes, thus recommending the adoption of future 3D-printed implants for total ankle replacement. Wu et al. [112] developed a 3D bioprinted scaffold consisting of rat bone marrow MSCs enclosed within a double hydrogel composed of gellan gel (GG) and polyethylene glycol diacrylate (PEGDA). This scaffold was designed to mimic the PLA framework for disc regeneration, serving as a microenvironment, and demonstrated excellent cell viability. Stents possessing viscoelastic properties have proven effective in promoting intervertebral disc healing. Li et al. [113] utilized in situ 3D bioprinting for the treatment of large bone defects in a preclinical animal model. The bio-ink formulation consisted of sodium alginate, PEGDA, GelMA, and I-2959 photoinitiator. Alginate crosslinking was achieved using CaCl2, while ultraviolet (UV) lamps with an intensity of 100 mW/cm2 were employed for photopolymerization. Intramuscular injection of cefuroxime sodium was administered post-implantation to prevent infection, and the animals were euthanized after a period of 12 weeks. MicroCT imaging and subsequent 3D reconstruction at this time point revealed enhanced reparative capacity in the animals treated with the 3D printed constructs, effectively filling the defect voids [110]. Li et al. [106] further verified the safety and effectiveness of TDN—CLI-loaded 3D bioprinted hybrid scaffolds through a series of in vitro and in vivo experiments, proving that this new scaffold has broad application prospects in the treatment of infectious bone defects (Fig. 4B).
6.
Conclusion and prospect
The personalized and targeted nature of 3D printing technology has revolutionized the biomedical field by offering tailored resolutions for different scenarios. This innovative technology enables the fabrication of precisely matched structures and target objects that cater to patients' specific needs, thereby leading to enhanced patient outcomes. In the realm of bone tissue engineering, 3D printing has emerged as a transformative tool. Researchers are actively investigating advanced scaffold materials capable of mimicking the inherent properties of bone, facilitating improved integration with surrounding tissues and augmenting regenerative capabilities. By meticulous control over factors such as porosity, mechanical strength, and bioactivity, 3D-printed scaffolds hold tremendous promise in enabling successful bone tissue regeneration.
The current application of 3D printing technology in the field of clinical medicine is still at its early stages, but it has shown great potential for revolutionizing healthcare. Personalized medicine, tailored to individual patients' needs and characteristics, can be delivered with the use of 3D printing technology. The realization of the application of 3D printing technology in clinical settings requires the integration of multiple factors. First, the preparation of the reported bone tissue engineering scaffolds is complex and costly, which limits the construction of related materials to laboratory scale [114]. Further improvements are needed in material diversity, with the goal being to achieve a high level of anthropomorphism in printed organ models, including materials and tactile properties that closely resemble human tissue. Additionally, there is a need for advancements in the biomechanical performance of 3D printed bones, as certain joint surfaces cannot currently be effectively printed using this technology, limiting its application in areas prone to wear. From initial ideas and attempts, personalized joint prostheses created through 3D printing have gradually evolved into a clinically mature application model with established technical specifications. This key technology has been independently innovated by Chinese doctors and has positioned China's personalized orthopedic medicine at the forefront of global medical advancements, particularly in bone tumor resection and reconstruction procedures. Following completion of preclinical studies, multicenter clinical trials are necessary to gather extensive data evaluating the safety and effectiveness of 3D printing technology for clinical applications. Clinical trials typically involve multiple phases starting from an initial safety assessment leading up to larger-scale demonstrations of effectiveness. Simultaneously, an application must be submitted to regulatory agencies responsible for medical devices; this process entails providing detailed technical documentation and clinical trial data as evidence supporting product safety and efficacy [115]. However, there are still challenges that need to be addressed before widespread implementation can take place. One major challenge lies in the unpredictability of outcomes when using 3D printing technology. While it offers immense possibilities for customization and precision, there is a need for further research and development to ensure consistent and reliable results. Clinical trials are essential to validate the effectiveness and safety of 3D printed medical devices or implants. Another obstacle is the high requirements imposed by 3D printing on materials, equipment, and environmental conditions. Existing materials often fall short in meeting these demands, resulting in various defects such as poor mechanical properties or limited biocompatibility. To overcome this limitation, ongoing efforts are being made to explore new materials that possess superior properties suitable for medical applications. In addition to seeking new materials, improving existing ones through surface modification techniques and composite approaches with other compatible materials is also crucial. Surface modifications can enhance biocompatibility while composite techniques allow for combining the strengths of different material into a single substance or device. Furthermore, enhancing the biological properties of different materials is necessary to optimize their performance within clinical settings. This includes various methods that aims at improving bioactivity (the ability to interact with living tissues), promoting cell adhesion and proliferation on surfaces, as well as preventing bacterial colonization or infection risks associated with implanted devices.
The research on the application of 3D printing technology in clinical medicine primarily focuses on orthopedic diseases in order to offer a practical and effective approach for bone regeneration and repair. However, further advancements are necessary to develop novel 3D printing products for treating other medical conditions. One area that holds great potential is the field of organ transplantation. With the shortage of donor organs worldwide, 3D printing technology could revolutionize this process by allowing for the creation of custom-made organs using a patient's own cells. This would not only eliminate the need for immunosuppressive drugs but also significantly reduce waiting time and improve patient outcomes. Moreover, researchers are exploring how 3D printing can be utilized in reconstructive surgery. By precisely replicating complex anatomical structures such as facial features or cranial bones, surgeons can achieve better aesthetic results while ensuring complete functional restoration, which is especially suitable for patients who have suffered from traumatic injuries or congenital deformities. In recent years, there has been significant progress in the development of 4D bio-printing technology, which enables programmable deformation ability in pattern structures through shape change and responsive characteristics to various biological materials. This technology allows for precise control and testing of individual variables, such as timed release of growth factors or regulation of cancer cell behavior within their environment by utilizing advanced 3D bio-printing processes and technologies [42]. The examples mainly encompass computer-aided design (CAD) modeling and 3D printers [116]. The incorporation of detailed pre-programmed modulation enables 4D printed structures to effectively achieve the desired temporal changes in response to specific stimuli, facilitated by scalable and flexible smart materials. The concept of 4D printing significantly enhances the scope and complexity of additive manufacturing [117] and the role of smart biomaterials is pivotal among them. With the advent of novel manufacturing materials, 3D printing of intelligent biomaterials will undergo structural or functional reconfiguration, thereby enabling this 4D-printed biological scaffold to exhibit intellectually controlled behavior, thus yielding enhanced advantages in the field of bone tissue engineering [117]. Extensive research has been conducted on natural and synthetic smart materials for physical, chemical, or biological stimulation in the field of bone repair [118].
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
CRediT authorship contribution statement
Jingwen Wang: Formal analysis, Data curation, Conceptualization. Peizhang Zhao: Formal analysis, Data curation. Mengmeng Li: Formal analysis, Data curation. Jun Li: Data curation. Yunfeng Lin: Writing – review & editing, Supervision, Conceptualization.
Acknowledgments
This study was supported by the National Natural Science Fund of China (Nos. 82202726, 82370929); the National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University (No. Z20192013); Key research and development project of Sichuan Science and Technology Department (No. 2023YFG0219); "ZerotoOne" Innovation Research Project of Sichuan University (No. 2022SCUH0014); Frontiers Medical Center, Tianfu Jincheng Laboratory Foundation (No. TFJC2023010001), Sichuan Science and Technology Program (No. 2022NSFSC0002), Sichuan Province Youth Science and Technology Innovation Team (No. 2022JDTD0021), Research and Develop Program, West China Hospital of Stomatology Sichuan University (Nos. RD03202302, RCDWJS2024-1).
Supplementary materials
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.cclet.2024.110686.
X. Chen, S. Han, W. Wu, et al., Small 18 (2022) e2106824.
[118]
P. Rastogi, B. Kandasubramanian, Chem. Eng. J. 366 (2019) 264–304.
Figure 1
(A) Examples of mechanisms through which coatings containing magnesia enhance osseointegration in implants involve the activation of transient receptor potential melastatin 7 (TRPM7) protein channels and magnesium ions within integrin, extracellular signal-regulated kinase pathway (ERK), wingless-type (WNT) MMTV integration site family member, and PI3K pathways. Reproduced with permission [23]. Copyright 2023, Elsevier. (B) The immune response to treatment with zinc-based materials involves the initial recognition of pathogens by neutrophils and monocytes. Subsequently, M1 macrophages undergo polarization into M2 macrophages, which then mediate the expression of anti-inflammatory factors, thereby participating in adaptive immunity. Finally, during the tissue healing phase, M2 macrophages secrete relevant factors that promote wound healing and reconstruction. Reproduced with permission [25]. Copyright 2023, Elsevier.
Figure 2
(A) Methods and pathways of iPSC generation and further differentiation into satellite cells. Reproduced with permission [79]. Copyright 2023, MDPI. (B) Major signaling pathways regulating self-renewal and pluripotency of human embryonic stem cells. Reproduced with permission [82]. Copyright 2023, MDPI.
Figure 3
(A) The utilization of additive manufacturing technology in the field of orthopedics. Reproduced with permission [92]. Copyright2022, Hindawi. (B) Future development of organ model 3D printing. Reproduced with permission [93]. Copyright 2021, Wiley.
Figure 4
3D bioprinting allows efficient production of complex bone structures. (A) 3D printed model after virtual fracture reduction. Appropriately customized plates and fracture 3D models are sterilized and on standby for use during surgery [107]. Copyright 2023, Nature. (B) The synthesis of TDN—CLI complex and the construction of TDN—CLI supported 3D bioprinting composite scaffold, show excellent antibacterial and osteogenic properties. Reproduced with permission [106]. Copyright 2022, Elsevier.

 DownLoad:
DownLoad:

 下载:
下载:





 下载:
下载:
