
Scheme 1.
DH desensitization therapy involves various biomaterials to achieve dentinal tubule closure and dental nerve blockade.
Dentin-desensitizing biomaterials
Qihui Wang , Jiayi Luan , Zhilong Zhao , Weihui Kong , Congxiao Zhang , Jianxun Ding

Dentin hypersensitivity (DH) is a common clinical symptom with the typical characteristic of a toothache induced by varying degrees of dentin exposure. Due to the lack of adequate evaluation criteria, the incidence of DH in different regions and populations shows considerable heterogeneity. According to the published results of random-effects meta-analyses, the incidence rate of DH is about 33.5% [1]. Existing studies have primarily focused on populations in Europe and Asia, university clinics, and community settings. The typical sharp toothache seen with DH arises from exposed dentin under various external stimuli that include temperature (hot or cold), chemicals (sour or sweet), and mechanical action (friction or mastication). Multifactorial etiologies cause dentin exposure, including physiological and pathological factors [2]. The most common physiological factor for dentin exposure is the physiological gap between the enamel and cementum. Tooth wear, wedge-shaped defect, tooth fracture, dental caries, periodontal atrophy, filling and noncompaction, tooth bleaching, and dental root leveling are essential pathological factors in the development of DH [3].
Dentin is composed of dentinal tubules, dentine fibers, and matrix. Dentinal tubules run through the whole dentin and are arranged radially from the dental pulp surface to the enamel-dentinal junction. Dentinal tubules contain nerves, blood vessels (Scheme S1A in Supporting information), odontoblasts processes, and dentinal fluid. Open dentinal tubules are visible on the exposed dentin surface. The number of open dentinal tubules in DH is eight times that of normal dentin, and their diameter is 2-fold [4].
The most widely accepted DH pathogenesis is Brannstrom's hydrodynamic theory [5-7]. Dentinal fluid flows under external stimulation, and odontoblast membranes are susceptible to dentinal fluid flowing and sudden pressure changes. Toothache arises from the relaxation and compression of odontoblasts and odontoblast processes, the mechanical deformation of nerve fibers, the broadening of sodium ion (Na+) channel, and fiber depolarization [8]. In addition, direct innervation theory and odontoblastic transduction theory further explain the pathogenesis of DH. Direct innervation theory holds nerve fibers extend from the dental pulp to dentinal tubules. The pulp nerves in exposed dentinal tubules transmit external stimuli through nerve endings, then finally transfer nerve signals to the brain center to report a toothache (Scheme S1B in Supporting information). The odontoblasts and their processes play a synaptic-like role in nerve transmission [9]. Adenosine triphosphate (ATP), neuropeptides, and glutamate are involved in toothache signal transduction as neurotransmitters [10]. Neuropeptides, such as substance P, neurokinin A (Scheme S1C in Supporting information), and calcitonin gene-related peptide (Scheme S1D in Supporting information) are increased under orthodontics, dental caries, and other external stimuli (Scheme S1E in Supporting information). Increased levels of neuropeptides are essential in the development of toothache [11-13]. Odontoblastic transduction theory mainly holds that odontoblast protrusions run through the dentin and eventually form enamel spindles at the enamel-dentinal junction. Odontoblasts contribute to toothache by mediating signaling through acetylcholine released after stimulation.
The exposed dentinal tubules are the effective targets for DH therapy. Dentinal tubule closure and dental nerve blockade are the ultimate goals of desensitization therapy [14]. Current clinical treatments, including medication, filling repair, laser irradiation, and desensitizing toothpaste are summarized in Table S1 (Supporting information). Desensitization medicines with low toxicity, such as sodium monofluorophos-phate gel, sodium fluoride (NaF) glycerin, NaF solution, strontium chloride (SrCl2), diamine silver fluoride [AgF: (NH3)2AgF] and silver iodide (AgI), can be easily applied to the exposed dentin surface [15-20]. However, saliva and chewing quickly remove any desensitizing medicine placed on the dentin surface. Improper application of silver nitrate (AgNO3) containing desensitizers carries the risk of staining teeth and burning oral soft tissue. Filling repair results in the loss of normal dental tissue and is only suitable for patients with DH symptoms with few teeth [16]. A high degree of tightness is essential for the margins of filling repair site, as poor tightness results in microleakage and secondary caries. Lasers with simple administration have an immediate desensitization effect. However, cracks on the dentin surface and possible damage to soft oral tissue limit their application. Desensitizing toothpaste can be used independently by patients to relieve DH but is also easily removed by acid, friction, and saliva stimuli, showing poor acid resistance, friction resistance, and stability.
Exposed dentinal tubules are constantly affected by a complicated oral environment, and deposition from desensitizing biomaterials in dentinal tubules is required to increase resistance to various stimuli. The composition and physical properties of deposits determine the effectiveness of dentinal tubule closure. In addition to an ability to penetrate dentinal tubules and achieve dental nerve blockade, desensitizing materials must also meet essential criteria proposed by American endodontist Grossman, as follows: no pulp stimulation, painless, easy administration, rapid action, and no tooth coloring. To date, researchers have examined numerous organic or inorganic biomaterials as possible effective desensitizing treatments. As a powerful weapon, biomaterials thrive in cardiovascular and cerebrovascular diseases, cancer, tissue damage, and DH. The synthesized biomaterials are easy to process to control their properties and biocompatibility. Compared with natural biomaterials and biologically inert materials, this avoids some restrictions and paves the way for more targeted applications. Biomaterials are viable therapeutic tools to address the shortcomings of current clinical strategies, hence achieving a long-lasting desensitization effect.
This review elucidates the mechanism of different desensitizing biomaterials in detail (Table S2 in Supporting information), such as reducing dentinal tubule diameter, ion precipitation, bionic mineralization, protein precipitation, and dental nerve blockade (Scheme 1). At the same time, the emerging opportunities of dentin regeneration biomaterials in the treatment of DH deserve deep exploration.
Based on Brannstrom's hydrodynamic theory, direct innervation theory, and odontoblastic transduction theory, researchers have found that exposed dentinal tubules, nerves, blood vessels, and odontoblasts are involved in the development and progression of DH. Hence, the changing diameter and density of exposed dentinal tubules, effectively regulating the transmission of protein inside and outside the blood vessels, and blocking nerve signal transmission are considered the foci of desensitization treatment. Besides, desensitizing materials with acid resistance, friction resistance, and stability lay a foundation for realizing a long-term effective desensitization effect.
The sealing rate and depth of dentinal tubules are significant in DH therapy. Modulating dentinal tubule deposition behaviors via biomaterials is promising in dentinal tubule closure. Significant goals in effective desensitization conclude reducing the diameter of dentinal tubules, forming ion precipitation via a desensitizing coating, promoting bionic mineralization, and protein exudation and coagulation in dentinal tubules. Mechanisms of different desensitizing materials capable of regulating dentinal tubule closure are summarized in Table S2 (Supporting information).
Lasers have been applied to treat various oral diseases, including dental caries, oral mucosal diseases, pulpitis, and DH. Lasers, such as the diode laser, the neodymium-doped yttrium aluminum garnet (Nd: YAG) laser, the neodymium-doped yttrium aluminum perovskite (Nd: YAP) laser, the erbium: yttrium-scandium-gallium-garnet (Er: YSGG) laser, the erbium: yttrium-aluminum-garnet (Er: YAG) laser, the erbium, chromium: yttrium-scandium-gallium-garnet (Er, Cr: YSGG) laser, the carbon dioxide (CO2) laser, helium-neon (He-Ne) laser, and the gallium aluminum arsenide (GaAlAs) laser are commonly used in DH therapy [18,21-44]. The treatment effectiveness rate of He-Ne laser ranges from 5.2% to 100%, GaAlAs laser ranges from 53.3% to 94.2%, CO2 laser ranges from 59.8% to 100%, Nd: YAG laser ranges from 5.2% to 100%, and Er: YAG laser reportedly ranges from 38.2% to 47%. Meanwhile, Er, Cr: YSGG laser keeps desensitizing stability for three months [45].
These lasers have the potential ability to achieve dentinal tubule closure and relieve DH. Lasers transmit light energy to heat up and melt the dentin surface, and then, a double-layered tubule structure is formed to reduce the diameter of exposed dentinal tubules. Halving the diameter of dentinal tubules minimizes the amount of dentinal fluid in dentinal tubules by up to 16 times [46]. Besides, lasers evaporate dentinal fluid and deposit insoluble salt in dentinal fluid, reducing the movement of dentinal fluid [47]. However, some researchers have proposed that lasers cannot completely occlude dentinal tubules and play a specific role in reducing their diameter.
The CO2 laser reduces the diameters of dentinal tubules by melting and solidifying the dentin surface. However, CO2 irradiation results in dentinal cracks and collagen fiber degradation. To achieve a better desensitization effect, researchers have applied laser and desensitizing agents like bioactive glass (BG) to exposed dentinal tubules simultaneously. BG acts with dentin to form an amorphous hydroxyapatite (HA) layer on the dentin surface to seal exposed dentinal tubules [39,48-50]. The simultaneous application of CO2 laser and BG paste prevents crack formation and collagen fiber degradation [51]. BG also completely dissolves and penetrates dentinal tubules under Nd: YAP laser irradiation. Specifically, the Si-O-Si bond of BG is broken and polymerized, which induces the enrichment of calcium (Ca) and phosphorus (P) and promotes the adhesion of BG to the walls of dentinal tubules, thus achieving effective DH therapy [28]. In addition to BG, various desensitizers, such as Gluma® (GD; Heraeus, Germany), Teethmate desensitizer (TMD; Kuraray Noritake Dental Inc., Tokyo, Japan), and photothermic agents, could be used together with lasers to obtain a better desensitization function [25,52]. Desensitizing agents play a critical role in assisting laser desensitization, reducing the diameter of dentinal tubules, and avoiding crack formation on the dentin surface. The dentin surface is heated and carbonized by absorbing laser energy. Desensitizers absorb part of the laser energy, which helps prevent irreversible damage to dentin caused by high temperature. Besides, desensitizing agents are melted, absorbed and transformed, and crystallized and recrystallized under laser irradiation. The synergistic effect of laser and desensitizer improves the acid resistance of DH therapy.
DH treatments with appropriate wavelengths and frequencies of lasers—such as treatments with Nd: YAG laser at 1064.0 nm and 1.5 W, Er: YAG laser at 60.0 mJ/pulse and 2.0 Hz, CO2 laser at 10, 600.0 nm and 1.0 W, diode laser at 810.0 nm and 1.5–2.5 mW, Nd: YAP laser at 1340.0 nm and 30.0 Hz, and Er, Cr: YSGG laser at 2780.0 nm and 0.25 W—play a significant role in dentinal tubule closure [28,32,33,44,51]. However, the wavelengths and frequencies of these lasers are not immutable, and more effective wavelengths and frequencies of lasers are worthy of further exploration. Moreover, laser security deserves more attention. Previous researches suggest that the thermal energy generated by laser application damages the periodontium and dental pulp tissue, and the thermal change damage threshold for periodontal ligaments is 7 ℃, and that for dental pulp is 3 ℃ [53,54].
Tooth brushing controls plaque and dental calculus, thus preventing dental caries and periodontal disease. Therefore, it is feasible to add desensitizing agents to toothpaste. Various desensitizing agents in marketed toothpaste, including potassium nitrate (KNO3), NaF, stannous fluoride (SnF2), calcium sodium phosphate silicate (CSPS), calcium phosphate (Ca3(PO4)2), Sr, arginine nanomaterials, and so forth, have the ability to occlude dentinal tubules [55-63]. Desensitizing toothpaste agents could be deposited into dentinal tubules as a continuous, uniform coating on the dentin surface.
HA is the main component of dentin, whose use has been reported to promote enamel remineralization, tooth whitening, and desensitizing [64-66]. The Ca/P ratio in the HA is 1.67, reveals the composition of inorganic components in dental tissue. The change of Ca/P ratio on the dentin surface may change the proportion of organic/inorganic components, eventually achieving dentin permeability change. Desensitizers with poor acid resistance can be dissolved by acid etching, resulting in the re-exposure of dentinal tubules. Crystalline biomimetic HA could be deposited on the dentin surface, even after acid etching [67]. The diameter of dentinal tubules ranges of 0.9–2.5 µm. HA particles with smaller diameters penetrate dentinal tubules more easily. Therefore, toothpaste containing nano-sized HA (nano-HA) had a better desensitizing effect than micron-sized HA (micron-HA), and toothpaste containing 80 nm of HA was more effective in sealing dentinal tubules than that containing 300 nm of HA [68]. HA dissolved in dentinal fluid to form a highly saturated Ca and P environment. The released ions continued to enter dentinal tubules to shape sediment and occlude dentinal tubules. Micro-HA particles had a smaller contact surface area with dentinal fluid than nano-HA particles. Therefore, it was difficult for micron-HA particles to degrade to form a Ca- and P-rich environment. At the same time, the chemical activity of nano-HA particles surface makes them tightly adhere to dentinal tubules, which is significant in resisting external stimuli and improving the Ca/P ratio of the dentin surface.
Fluoride elements in toothpaste replace hydroxyl groups of HA to form fluorapatite (FAp). FAp is difficult to dissolve. Hence, the chemical stability and acid resistance of FAp are better than those of HA in a complex oral environment. Fluoride increases the degree of dentin mineralization and forms an obvious high-density mineralization area on the dentin surface [69,70]. In research, a multi-benefit SnF2-based toothpaste stabilized with zinc (Zn) and P immediately sealed dentinal tubules by > 80%. The tin (Sn2+), zinc (Zn2+), phosphate (PO43−), and silicon ions (Si4+) of the toothpaste deposited on the dentin surface and formed a desensitizing coating to realize dentinal tubule closure [71]. Elsewhere, the Ca2+, fluoride ion (F−), and Zn2+ of a unique fluorozinccalsiumsilicate-based desensitizer (CAREDYNE Shield, GC Dental Industrial Corporation, Tokyo, Japan) were deposited in dentinal tubules, and the ion precipitation on the dentin surface sealed dentinal tubules effectively [72]. Besides, Zn2+ inhibits the degradation of dentin collagen and reduces the occurrence of dentin demineralization [73]. During experiments, AgF: (NH3)2AgF blackened teeth due to Ag precipitation, but replacing Ag with Si promoted the formation of apatite and did not stain teeth. Elsewhere, the formation of Si-Ca P complex precipitation by ammonium hexafluorosilicate (SiF: (NH4)2SiF6) realized dentinal tubule closure [74]. Meanwhile, calcium fluoride (CaF2) added to toothpaste continuously releases F− to promote the formation of low-solubility FAp, which is beneficial to the treatment of DH [75].
These desensitizing materials achieve dentinal tubule closure by releasing ions into dentinal tubules. Desensitizing materials shape a coating on the dentin surface, which continues imbuing ions into dentinal tubules that bind closely to the walls of dentinal tubules, and ion precipitation eventually occludes exposed dentinal tubules. However, bionic remineralization promotes the formation of mineralization. The structure of mineralization is closer to dentin tissue, which has better acid resistance, friction resistance, and stability than ion precipitation. More information is shown in Supporting information (Section S1, Ion precipitation).
Ion precipitation plays a specific role in relieving DH. However, due to the poor acid resistance and stability of desensitizing agents, simple brushing and ion deposition lead to a short-term desensitization effect in patients with severe DH. Therefore, developing a desensitizer with a noticeable desensitization effect and a long-term stable effect is essential. Based on the Grossman desensitizer standards, most researchers have devoted themselves to developing biomimetic analogs that promote the nucleation and growth of HA. Polydopamine (PDA), chitosan, poly(ethylene glycol) (PEG), biomimetic self-assembled peptide, copine-7 (CPNE7), BG, and mesoporous silica (MSN) play significant roles in the formation of HA [76-78]. Biomimetic analogs penetrate the deep layer of dentinal tubules owing to their small molecules and promote the conversion of Ca2+ and HPO42- into HA, the precipitates with acid and friction resistance bind tightly to the walls of dentinal tubules. Thus, biomimetic analogs have considerable prospects for long-term desensitization. Dentinal remineralization is an ideal method for DH therapy. Lima et al. compared the desensitizing effects of PDA, poly(3,4-dihydroxy-L-phenylalanine) (DOPA), poly(caffeic acid), and a synthesized DOPA-peptide possessing collagen Ca-binding domains (DOPA-Ahx-(Gly)3-(Glu)5) [79,80]. Catechol molecules in these compounds promoted the remineralization of HA in the orifice and inner walls of dentinal tubules. The progress of dentinal remineralization mainly involved oxidation containing catechol molecules, binding to exposed collagen fibers and crystal nucleation. However, this research did not confirm the responses of materials to acid and friction.
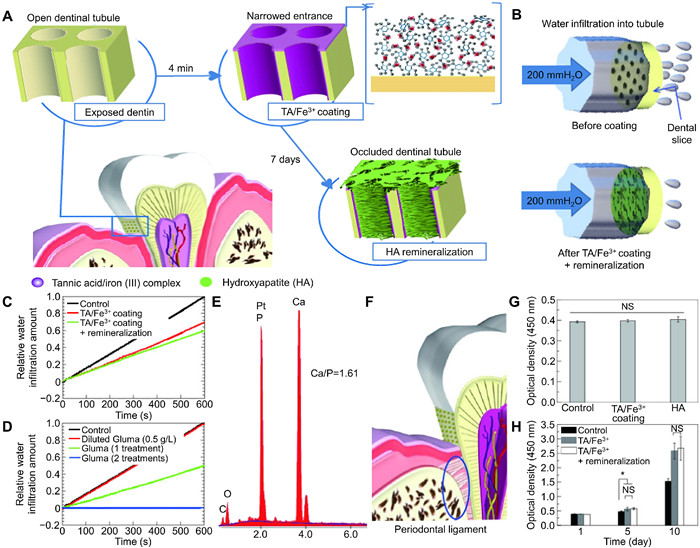
Oh et al. proposed a tannic acid iron(Ⅲ) (TA/Fe3+) complex, which formed a composite film on the dentin surface to significantly reduce the dentinal permeability (Figs. 1A and B) [81,82]. It was exciting to observe that the film withstood mechanical friction. The characteristic purple color on the dentin surface confirmed the special targeting of TA/Fe3+. The effectiveness of Gluma® in DH therapy has been proven in clinical studies. The change in dentinal permeability after treatment with TA/Fe3+ was similar to that seen after a single treatment with Gluma® (Figs. 1C and D). After soaking in saliva for seven days, needle-like HA crystals (Fig. 1E) could still be found densely and uniformly filled with dentinal tubules. A low concentration of TA/Fe3+ still has high binding energy in water. A gap between the enamel and cementum leads to the exposure of internal dentin. Therefore, the atrophy of periodontal tissue exacerbates dentin exposure in the oral environments (Fig. 1F). The TA/Fe3+ complex provides suitable conditions for the growth of fibroblasts and promotes the periodontal tissue regeneration (Figs. 1G and H). The renewal of periodontal tissue has a significant assistant role in dentinal tubule closure.
The desensitization mechanism of a gallic acid (GA)/metal ion complex was similar to that of TA/Fe3+. In research, robust and reversible GA/metal complexes, including Sr2+, Ca2+, Fe3+, titanium dioxide (TiO2), iron(Ⅲ) oxide (Fe2O3), and silicon dioxide (SiO2), adhered to the dentin surface to form HA nucleation sites, which were used as cores of remineralization to form dense HA crystals. Due to the stability of the GA/Fe3+ complex, the octahedral complex displayed the fastest deposition rate and highest sealing rate of dentinal tubules, so Fe3+ stood out from other metal ions or metal oxides [83]. GA/Fe3+ overcame the disadvantages of the long incubation time of TA with saliva and the poor color effect of TA/Fe3+. The sealing result of GA/Fe3+ was also better than that of the TA/Fe3+ complex. Pyrogallol moieties were bound to Ca2+, so the pyrogallol moieties in GA might be considered responsible for the nucleation of anisotropic growth of HA. GA/Fe3+ promoted the proliferation of periodontal tissue cells, showing good biocompatibility and an auxiliary desensitization effect.
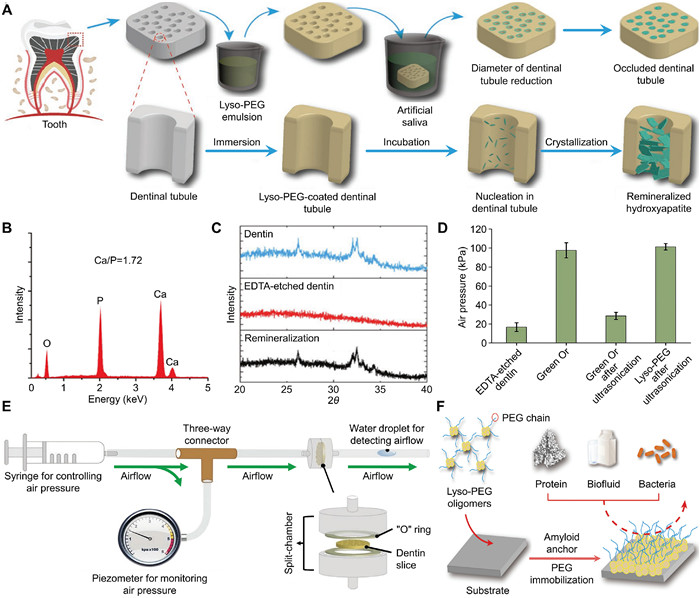
Chitosan, a natural polymer obtained via the deacetylation of chitin, promotes the remineralization of acid-etched dentin and increases the retention of tin salts and fluoride on demineralized tooth structures [84,85]. Carboxymethyl chitosan (CMC) and lysozyme (LYZ) form a nanogel through electrostatic interaction. Amorphous calcium phosphate (ACP) is involved in the formation of HA in the process of biomineralization. Thus, loading ACP onto nanogel promoted dentin biomimetic remineralization. At the same time, CMC takes part in improving the stability of ACP in solutions. In research, the CMC/LYZ-ACP nanogel deposited Ca2+ and PO43− onto the dentin surface to form HA mineralization, and the mineralization was tightly bound to dentinal tubules. Mineralization and natural dentin have similar properties, hardness values, and elastic moduli [86]. LYZ-PEG had an application prospect in DH therapy [87]. In this research, LYZ-PEG oligomer emulsion spreaded rapidly with strong adhesion on the dentin surface, and the participation of LYZ triggered the material to form amyloid aggregation and promoted the formation of a solid PEG-lated nanofilm on the dentin surface. Functional groups, such as carboxyl, hydroxyl, and amino groups on the nanofilm surface, supported the chelation of Ca2+ and HPO42- and formed a desensitizing layer on the walls of dentinal tubules to promote dentin remineralization (Fig. 2A). The Ca/P ration and X-ray diffraction (XRD) data revealed that the main component of remineralization layer was HA (Figs. 2B and C). The sealing depth of LYZ-PEG in dentinal tubules was calculated to be up to 60 ± 5 µm. A dentin slice treated with Lyso-PEG retained dentinal tubule closure after ultrasonication, and the air permeation test showed that the dentin slice had the characteristic of air pressure resistance (Figs. 2D and E). Green OrTM desensitizer with poor mechanical resistance could not penetrate the deep depth of dentin, so it could not withstand ultrasonication. The nanofilm had the characteristics of protein, biofluid, and bacteria resistance (Fig. 2F), so it was not affected by extreme pH, organic solvent, and protease and overcame the shortcomings of poor long-term desensitizing effect, poor stability, and insufficient sealing depth.
BG (P2O5-Na2O-CaO-SiO2) is currently used in many fields, such as angiogenesis, inflammation, bone repair, periodontal disease, and DH [88-91]. BG has a long-term remineralization effect and good biological activity [92]. In experiments, nano-BG formed apatite rods in dentinal tubules that were mechanically chimeric with dentin, achieving a stable desensitization effect [93,94]. Elsewhere, the apatite layer formed by nano-structured sol-gel BG on the dentin surface realized the chemical combination between the material and dentin. It revealed that materials remained bound to dentin even after being brushed or repeatedly soaked in an acid solution [95]. A unique multi-component BG, SiO2-P2O5-CaO-CaF2-SrO-SrF2-ZnO-Na2O-K2O with increasing CaF2 and SrF2 content, released F− and potassium ion(K+) on the dentin surface to occlude dentinal tubules [96]. Nd: YAP laser application assisted BG in improving the desensitization effect [28]. Moreover, dental pulp-derived mesenchymal stem cells (DP-MSCs), a crucial factor in dentin mineralization, differentiated into the dentin structure using BG and laser application [97].
MSN materials have shown excellent properties in the field of desensitization. Calcium carbonate@mesoporous silica (CaCO3/CCMS) was mixed with 30% phosphoric acid (H3PO4) to form CCMS-HP (Fig. S1A in Supporting information), which released Ca2+ into dentinal tubules and absorbed Ca2+ from the surrounding microenvironments to form mineralization in dentinal tubules, resulting in an increasing ratio of Ca/P in dentinal tubules. Dicalcium phosphate dehydrates (DCPD), tricalcium phosphate (TCP), and HA crystals are found in dentinal tubules at a depth of approximately 40 µm [98]. CaHPO4 precipitate formed upon mixing CCMS and H3PO4 (Fig. S1B in Supporting information). However, due to the unique structures of dentinal tubules and complex oral environments, crystal formation may be slightly different. The alkaline phosphatase (ALP) assay reveals that CCMS-HP has the potential ability to induce the activity of ALP through the dentin. Meanwhile, CCMS-HP utilizes the remineralization ability of DP-MSCs to achieve dentin remineralization (Fig. S1C in Supporting information). Ca3(PO4)3 formed along the walls of dentinal tubules instead of forming a desensitizing layer at the dentinal tubule orifice to block external stimuli (Fig. S1D in Supporting information). The coating will block the continuous penetration of ions.
Ionic precipitation DH therapy mainly deposits ions to the surface and interior of dentinal tubules and achieves transient and poorly stable dentinal tubule closure. Bionic remineralization has a promising prospect in DH therapy due to exhibiting long-term and sound desensitizing effects. HA nucleation and growth can be induced by simulating an oral environment, introducing functionalized groups, and providing mineralized molds. Biomimetic analogs penetrate the deep layer of dentinal tubules due to their small molecules. While promoting the conversion of Ca2+ and HPO42- into HA, the mineralized material shows acid and friction resistance and is tightly integrated with the walls of dentinal tubules. Thus, biomimetic mineralization holds considerable promise to achieve a long-term desensitizing effect. More information is shown in Supporting information (Section S2, Bionic remineralization).
Most desensitizers mainly form crystals or barriers in dentinal tubules to reduce dentinal permeability and achieve a practical desensitizing effect. In addition to various ions, dentinal tubule fluid contains plasma protein, non-collagenous protein. Desensitizers use the characteristics of dentinal tubules containing protein components to achieve effective desensitization by precipitating plasma protein in dentinal tubules. Non-collagenous proteins mainly take part in dentin mineralization.
The polymerization of Admira Protect resulted in the precipitation of plasma proteins from dentinal tubules, and an intratubular septum layer formed in the lumen of dentinal tubules, thereby reducing the dentinal permeability and dentinal fluid flow [99]. Gluma® contains 3% glutaraldehyde and 35% hydroxyethyl methacrylate (HEMA) [100,101]. Treatment of DH with Gluma® relieved toothache immediately [49]. The glutaraldehyde in Gluma® induced plasma protein precipitates into dentinal tubules. A diaphragm was formed in dentinal tubules under physiological conditions to isolate bacteria and protect the dental pulp from external stimulation [102]. However, the degradation of HEMA led to Gluma® with poor acid resistance and stability.
Ag nitrate acted like Gluma® by promoting the protein deposition released from vascular sources to occlude dentinal tubules. As mentioned above, silver nanoparticle-loaded and nonporous silica-encapsulated mesoporous silica (Ag-MSNs@nSiO2) deposited Ag ions to seal dentinal tubules. However, the maintenance of the desensitization effect depended on continuous protein aggregation [103].
The complete closure of dentinal tubules blocks external stimuli from acting on the deep nerves, which assists in nerve desensitization. Therefore, some researchers consider nerve signal blockade to be an effective target for the treatment of DH. The disruption of transient receptor potential (TRP) channels, TREK-1 (K+ channel), Na+ channel, Ca2+ channel, and ATP activation on odontoblasts and dental primary afferent neurons are considered essential targets for achieving analgesia [10,104-107].
TRP, TREK-1, Na+, and Ca2+ channels are sensitive to mechanical stimulation, and mechanical stimulation is converted into electrical signals to activate them. The intracellular Ca concentration increases, and odontoblasts release ATP. The closure of dentinal tubules reduces the activation of channels by mechanical stimulation.
The GaAlAs laser transmits a portion of irradiation energy to the nerve for transient desensitization [44]. In experiments, this laser prevented C fibers from experiencing afferent depolarization, improved the pain threshold, and showed an immediate analgesic effect. TRP transmits various external stimuli, such as temperature and pressure. The Er, Cr: YSGG laser disrupted the TRP channels to achieve rapid desensitization [108]. Bacteria penetrated dentinal tubules via exposed dentin and reduce the pain threshold. Meanwhile, Er, Cr: YSGG laser application increased the toothache threshold by inhibiting bacteria and assisting desensitization. Therefore, the laser had a potentially significant role in relieving toothache [109,110].
K+ exists in most desensitizers, including desensitizing toothpaste, Desensibilize Nano P, Sensodyne® oral rinse (potassium chloride (KCl)), potassium oxalate desensitizer, D/sense® (Centrix Inc., Shelton, CT, USA), and other products with K salts [111-116]. K+ acts on nerve synapses through dentinal tubules, affecting nerve signal conduction, causing action potential inactivation, and ultimately relieving toothache. The ability of potassium citrate to relieve toothache was better than that of potassium oxalate, and that of potassium oxalate was better than those of KNO3 and KCl [117,118]. Many studies have confirmed the effectiveness of K+ in DH therapy. However, there are various obstacles to inhibiting the role of K+ in vivo. With the consumption of K+, toothache is increased, and researchers have questioned the desensitization effect of K+.
With the deepening of the research, McCormack et al. proposed an indirect analgesic effect of the second messenger nitric oxide (NO) based on the comprehensive analysis of effectiveness of K+ [119]. Researchers have confirmed the auxiliary role of NO in desensitization therapy. Only a tiny amount of K+ is required to induce NO synthesis, and inducible NO synthase (iNOS) within odontoblasts causes a sustained release of NO. The desensitization effect of applying a low-pH sodium chloride (NaCl) solution after thoroughly cleaning the dentin surface appeared better than that of monohydrogen-monopotassium oxalate. Researchers have proposed that an acidic salt solution may have an analgesic effect [120]. However, the specific mechanism of action is still unclear.
Treating DH is a highly elusive clinical challenge in dentistry. Long-term, effective control of dentinal tubule openings is critical for successful DH therapy. However, the clinical applications of existing strategies with poor acid resistance, friction resistance, and stability hindered by the complicated oral environments, and the desensitization effect are unsatisfactory. Therefore, it is necessary and urgent to develop advanced strategies or improve the efficiency of current treatments. Elucidating the pathogenesis of DH lays the cornerstones for developing innovative and effective therapeutic strategies. There has been promising progress made in developing biomaterials that regulate dentinal tubule closure and dental nerve blockade in the past few years. Different biomaterials have shown advantages and disadvantages in DH therapy by reducing dentinal tubule diameter, forming ion precipitates, promoting bionic mineralization, forming protein residues, and blocking nerve conduction.
The desensitization of laser with short administration is rapid and effective. However, the frequency and wavelength of laser should be carefully regulated to avoid forming dentin cracks and soft tissue damage. The laser can be applied simultaneously with desensitizers to prevent dentin cracks. Desensitizers shape a coating on the dentin surface and release ions into dentinal tubules to form ion precipitation that achieves mechanical occlusion without adhesion. However, due to the poor acid and friction resistance and poor stability, ions show a short-lived desensitization effect in the face of a complex oral environment. Hence, the formation of bionic remineralization is of particular importance. The mineralization is formed inside dentinal tubules by desensitizing agents. It resembles the dentin components and achieves strong adhesion to dentin to maintain stable desensitization in the face of acid, friction, and saliva. Nerves and blood vessels within dentinal tubules located in the deep layer of dentinal tubules, desensitizers must have an absolute particle size advantage, be able to enter the deep layer of dentinal tubules, and have the ability to act on nerves and blood vessels. Nerve blockade can fundamentally resolve the toothache of DH. However, with the consumption of ions, toothache relief gradually diminishes and be faced with a new round of toothache in the future.
HA is the main component of dentin, and biomaterials that promote HA remineralization have attracted much attention in DH therapy. Consequently, under ideal conditions, we will be able to tailor biomaterials for dentin regeneration to improve the speed and quality of desensitization. The chemical and physical properties of biomaterials, such as hardness, adhesion, and functional groups, can be adjusted for better desensitization. Mineralization is formed by biomimetic remineralization, and dentin is integrated to resist external stimuli and prevent external stimuli from acting on nerves through dentinal tubules, thus eventually eliminating toothache.
In conclusion, during the desensitizing process, dentinal tubule closure and dental nerve blockade are essential goals for complete desensitization. Any stimulation conditions that disrupt the sealing effect may reverse the desensitization effect. The development of biomaterials offers more advanced and promising treatment strategies to compensate for the deficiency of clinical therapeutic approaches. Under differentiated and complex pathophysiological conditions, future research on biomaterials should focus on the precise regulation of dentin regeneration. Based on the basic structure of normal dental tissue, the realization and application of biomaterials that simultaneously promote enamel and cementum regeneration is also a goal of future research. Research on the targeted regulation of biomaterials is still in its infancy. Future works should focus on combining the latest discoveries of advanced technologies in materials to realize precise regulation of the regeneration process of dental tissue. Hopefully, these biomaterials will provide higher efficiency for DH therapy in the foreseeable future.
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
This work was financially supported by the Special Program for Medical and Health Professionals of Jilin Province (No. JLSWSRCZX2021-085) and the Achievement Transformation Fund of the First Hospital of Jilin University (Nos. JDYYZH-2102055 and JDYYZH-2102013).
Supplementary material associated with this article can be found, in the online version, at
L.F. Zeola, P.V. Soares, J. Cunha-Cruz, J. Dent. 81 (2019) 1-6. doi: 10.1016/j.jdent.2018.12.015
K. Bekes, M.T. John, H.G. Schaller, C. Hirsch, J. Oral Rehabil. 36 (2009) 45-51. doi: 10.1111/j.1365-2842.2008.01901.x
J. Cunha-Cruz, J.C. Wataha, L.J. Heaton, et al., J. Am. Dent. Assoc. 144 (2013) 288-296. doi: 10.14219/jada.archive.2013.0116
T. Oyama, K. Matsumoto, J. Endod. 17 (1991) 500-502. doi: 10.1016/S0099-2399(06)81798-X
M.V.O. Närhi, T.J. Hirvonen, M.O.K. Hakumäki, Acta Physiol. Scand. 115 (1982) 173-178. doi: 10.1111/j.1748-1716.1982.tb07062.x
P.A. Walters, J. Contemp. Dent. Pract. 6 (2005) 107-117. doi: 10.5005/jcdp-6-2-107
P.L. Jacobsen, G. Bruce, J. Contemp. Dent. Pract. 2 (2001) 1-12. doi: 10.1061/40582(2001)10
N. Vongsavan, B. Matthews, Arch. Oral Biol. 52 (2007) 640-647. doi: 10.1016/j.archoralbio.2006.12.019
D. Andrew, B. Matthews, J. Physiol. 529 (2000) 791-802. doi: 10.1111/j.1469-7793.2000.00791.x
A. Aminoshariae, J.C. Kulild, J. Endod. 47 (2021) 1696-1702. doi: 10.1016/j.joen.2021.07.011
M.A. Kido, T. Ibuki, A. Danjo, et al., Arch. Histol. Cytol. 68 (2005) 259-265. doi: 10.1679/aohc.68.259
S. Kim, J. Endod. 16 (1990) 48-53. doi: 10.1016/S0099-2399(06)81563-3
J. Caviedes-Bucheli, H.R. Muñoz, M.M. Azuero-Holguín, E. Ulate, J. Endod. 34 (2008) 773-788. doi: 10.1016/j.joen.2008.03.010
S. Maity, V. Priyadharshini, S. Basavaraju, J. Indian Soc. Periodontol. 24 (2020) 441-446. doi: 10.4103/jisp.jisp_500_19
J. Creeth, J. Gallob, F. Sufi, et al., BMC Oral Health 19 (2019) 1-9. doi: 10.1186/s12903-018-0701-5
B.K. Yadav, A. Jain, A. Rai, M. Jain, J. Int. Oral Health 7 (2015) 137-143.
Z.H. Xiong, L. Xia, L. Mei, G.Z. Han, Y.M. Chen, Chin. J. Stomatol. 46 (2011) 214-217.
F. Femiano, R. Femiano, A. Lanza, et al., Am. J. Dent. 26 (2013) 214-218.
I. Willershausen, D. Schulte, A. Azaripour, et al., Clin. Lab. 61 (2015) 1695-1701.
G.G. Craig, G.M. Knight, J.M. McIntyre, Aust. Dent. J. 57 (2012) 308-311. doi: 10.1111/j.1834-7819.2012.01700.x
A.S. Bakry, H. Takahashi, M. Otsuki, et al., J. Dent. Res. 90 (2011) 246-250. doi: 10.1177/0022034510387793
K. Ozlem, G.M. Esad, A. Ayse, U. Aslihan, Niger. J. Clin. Pract. 21 (2018) 225-230.
H. Zhuang, Y. Liang, S. Xiang, et al., J. Appl. Oral Sci. 29 (2021) e20200266. doi: 10.1590/1678-7757-2020-0266
S. Kurt, T. Kırtıloğlu, N.A. Yılmaz, E. Ertaş, H. Oruçoğlu, Lasers Med. Sci. 33 (2018) 1883-1890. doi: 10.1007/s10103-018-2546-1
E. Öncü, S. Karabekiroğlu, N. Ünlü, Microsc. Res. Tech. 80 (2017) 737-744. doi: 10.1002/jemt.22859
J.H. Wang, K. Yang, B. z. Zhang, et al., BMC Oral Health 20 (2020) 1-10. doi: 10.1186/s12903-019-0991-2
Q.Z. Cui, M.G. Wei, Z.D. Xiong, et al., Photobiomodul. Photomed. Laser Surg. 39: 6 (2020) 390-394. doi: 10.1089/photob.2019.4797
B.S. Lee, C.W. Chang, W.P. Chen, W.H. Lan, C.P. Lin, Dent. Mater. 21 (2005) 511-519. doi: 10.1016/j.dental.2004.08.002
V. Maximiano, A.C. Machado, R.M. Lopes, et al., J. Appl. Oral Sci. 29 (2021) e20200736. doi: 10.1590/1678-7757-2020-0736
A.C. Machado, V. Maximiano, C.P. Eduardo, et al., Photobiomodul. Photomed. Laser Surg. 37 (2019) 262-266. doi: 10.1089/photob.2018.4575
F.F. Küçükekenci, A.S. Küçükekenci, F. Çakici, Odontology 107 (2019) 186-189. doi: 10.1007/s10266-018-0385-y
A. Dilsiz, T. Aydin, V. Canakci, M. Gungormus, Photomed. Laser Surg. 28 (Supp. 2) (2010) S11–S17.
A. Sicilia, S. Cuesta-Frechoso, A. Suárez, et al., J. Clin. Periodontol. 36 (2009) 650-660. doi: 10.1111/j.1600-051X.2009.01433.x
F.A. Rizzante, R.M. Maenosono, M.A. Duarte, et al., J. Periodontol. 87 (2016) 320-326. doi: 10.1902/jop.2015.150444
R. Praveen, S. Thakur, M. Kirthiga, M. Narmatha, J. Conserv. Dent. 21 (2018) 495-499. doi: 10.4103/JCD.JCD_197_18
S. Oh, Y. Gu, H. Perinpanayagam, et al., Lasers Med. Sci. 33 (2018) 1237-1244. doi: 10.1007/s10103-018-2464-2
H.B. Kara, U. Cakan, B. Yilmaz, P.I. Kurugol, J. Esthet. Restor. Dent. 28 (2016) 405-411. doi: 10.1111/jerd.12230
P.I. Demydova, J. Stomatol. 73 (2020) 170-175. doi: 10.5114/jos.2020.98312
L.M.S. Al-Saud, H.N.A. Al-Nahedh, Oper. Dent. 37 (2012) 340-355. doi: 10.2341/10-188-L
A. Dilsiz, T. Aydın, G. Emrem, Photomed. Laser Surg. 28 (Supp. 2) (2010) S69–S74.
K. Orhan, U. Aksoy, D.C. Can-Karabulut, A. Kalender, Lasers Med. Sci. 26 (2011) 591-598. doi: 10.1007/s10103-010-0794-9
A.L. Marsilio, J.R. Rodrigues, A.B. Borges, J. Clin. Laser Med. Surg. 21 (2003) 291-296. doi: 10.1089/104454703322564505
M.S. Noya, R.B. Bezerra, J.L. Lopes, A.L.B. Pinheiro, J. Appl. Oral Sci. 12 (2004) 363-366. doi: 10.1590/S1678-77572004000400021
H.G. Yilmaz, S. Kurtulmus-Yilmaz, E. Cengiz, H. Bayindir, Y. Aykac, J. Dent. 39 (2011) 249-254. doi: 10.1016/j.jdent.2011.01.003
M. Asnaashari, M. Moeini, J. Lasers Med. Sci. 4 (2013) 1-7.
D. Mehta, V. Gowda, W.J. Finger, K. Sasaki, Dent. Mater. 31 (2015) 1298-1303. doi: 10.1016/j.dental.2015.08.162
H.G. Yilmaz, E. Cengiz, S. Kurtulmus-Yilmaz, B. Leblebicioglu, J. Clin. Periodontol. 38 (2011) 341-346. doi: 10.1111/j.1600-051X.2010.01694.x
A.O. Lopes, C. d. P. Eduardo, A.C.C. Aranha, Lasers Med. Sci. 32 (2017) 1023-1030. doi: 10.1007/s10103-017-2203-0
A.O. Lopes, C. d. P. Eduardo, A.C.C. Aranha, Lasers Med. Sci. 30 (2015) 823-829. doi: 10.1007/s10103-013-1441-z
A.O. Lopes, A.C.C. Aranha, Photomed. Laser Surg. 31 (2013) 132-138. doi: 10.1089/pho.2012.3386
E.M.R. Lee, R. Borges, J. Marchi, C. d. P. Eduardo, M.M. Marques, J. Biomed. Mater. Res. 108 (2020) 939-947. doi: 10.1002/jbm.b.34446
H.Q. Gao, L.R. Zhang, X.L. Lian, et al., Mater. Chem. Front. 5 (2021) 3388-3395. doi: 10.1039/d0qm01006e
L. Zach, G. Cohen, Oral Surg. Oral Med. Oral Pathol. 19 (1965) 515-530. doi: 10.1016/0030-4220(65)90015-0
J.J. Sauk, K. Norris, R.A. Foster, J.M. Moehring, M.J. Somerman, J. Oral Pathol. Med. 17 (1988) 496-498. doi: 10.1111/j.1600-0714.1988.tb01323.x
M. Toledano, R. Osorio, E. Osorio, et al., J. Mech. Behav. Biomed. Mater. 68 (2017) 62-79. doi: 10.1016/j.jmbbm.2017.01.026
M. Toledano-Osorio, E. Osorio, F.S. Aguilera, et al., Acta Biomater. 72 (2018) 371-380. doi: 10.1016/j.actbio.2018.03.033
S.L. Tan, S.S. Chen, Y.F. Wang, et al., Dent. Mater. 36 (2020) 816-825. doi: 10.1016/j.dental.2020.03.028
P. Usai, V. Campanella, G. Sotgiu, et al., Nanomaterials 9 (2019) 1748-1757. doi: 10.3390/nano9121748
M.J. Zhu, J.L. Li, B. Chen, et al., PLoS One 10 (2015) e0140176. doi: 10.1371/journal.pone.0140176
N.X. West, T. He, Y.S. Zou, et al., J. Dent. 105 (2021) 103566. doi: 10.1016/j.jdent.2020.103566
J. Creeth, R. Maclure, J. Seong, et al., J. Clin. Periodontol. 46 (2019) 1105-1115. doi: 10.1111/jcpe.13175
S.H. Joao-Souza, L.O. Sakae, A. Lussi, et al., Clin. Oral Investig. 24 (2020) 2051-2060. doi: 10.1007/s00784-019-03069-7
Z.Y. Yang, F. Wang, K. Lu, Y.H. Li, Z. Zhou, Clin. Cosmet. Investig. Dent. 8 (2016) 1-14. doi: 10.1155/2016/6136178
R. Monterubbianesi, V. Tosco, T. Bellezze, et al., Materials 14 (2021) 3072-3082. doi: 10.3390/ma14113072
B.M. Souza, L.P. Comar, M. Vertuan, et al., Caries Res. 49 (2015) 499-507. doi: 10.1159/000438466
P.Y. Yuan, X.Q. Shen, J. Liu, et al., PLoS One 7 (2012) e45283. doi: 10.1371/journal.pone.0045283
L.D. Esposti, A.C. Ionescu, E. Brambilla, A. Tampieri, M. Iafisco, Materials 13 (2020) 2928-2940. doi: 10.3390/ma13132928
P.Y. Yuan, S.Y. Liu, Y.T. Lv, et al., Int. J. Nanomed. 14 (2019) 5243-5256. doi: 10.2147/ijn.s205804
A.R. PradeepKumar, V. Viswanath, K. Singh, et al., J. Conserv. Dent. 22 (2019) 522-528. doi: 10.4103/jcd.jcd_22_20
S.J. Khunkar, S. Utaka, I. Hariri, et al., Arch. Oral Biol. 60 (2015) 574-581. doi: 10.1016/j.archoralbio.2015.01.001
D. Hines, S.Y. Xu, M. Stranick, J. Am. Dent. Assoc. 150 (2019) S47-S59. doi: 10.1016/j.adaj.2019.01.006
T. Matsuura, M. Mae, M. Ohira, et al., Trials 21 (2020) 1-6. doi: 10.1080/23320885.2019.1704290
A. Saad, T. Nikaido, A. Abdou, et al., Dent. Mater. J. 38 (2019) 940-946. doi: 10.4012/dmj.2018-352
T. Suge, A. Kawasaki, K. Ishikawa, T. Matsuo, S. Ebisu, Dent. Mater. 24 (2008) 192-198. doi: 10.1016/j.dental.2007.03.009
D.S. Brauer, N. Karpukhina, M.D. O'Donnell, R.V. Law, R.G. Hill, Acta Biomater. 6 (2010) 3275-3282. doi: 10.1016/j.actbio.2010.01.043
Y. Cao, M.L. Mei, J.G. Xu, et al., J. Dent. 41 (2013) 818-825. doi: 10.1016/j.jdent.2013.06.008
Q.Q. Wang, S.Q. Wang, T. Zhao, et al., J. Appl. Biomater. Funct. Mater. 19 (2021) 33784188.
Y.H. Park, C. Son, Y.M. Seo, et al., Front. Cell Dev. Biol. 9 (2021) 655498. doi: 10.3389/fcell.2021.655498
J. Figueiredo-Macedo-de-Lima, M. d. C. Aguiar-Jordão-Mainardi, R.M. Puppin-Rontani, et al., Dent. Mater. 36 (2020) 501-511. doi: 10.1016/j.dental.2020.01.012
Y.Z. Zhou, Y. Cao, W. Liu, C.H. Chu, Q.L. Li, ACS Appl. Mater. Interfaces 4 (2012) 6901-6910. doi: 10.1021/am302041b
D.X. Oh, E. Prajatelistia, S.W. Ju, et al., Sci. Rep. 5 (2015) 1-8.
A.K.B. Bedran-Russo, K.J. Yoo, K.C. Ema, D.H. Pashley, J. Dent. Res. 88 (2009) 807-811. doi: 10.1177/0022034509342556
E. Prajatelistia, S.W. Ju, N.D. Sanandiya, et al., Adv. Healthc. Mater. 5 (2016) 919-927. doi: 10.1002/adhm.201500878
A. Zaharia, V.G. Plescan, E.M. Anghel, V. Musat, Rev. Chim. 68 (2017) 928-932. doi: 10.37358/rc.17.5.5583
N.I.P. Pini, D.A.N.L. Lima, J.R. Lovadino, C. Ganss, N. Schlueter, Caries Res. 50 (2016) 337-345. doi: 10.1159/000445758
J.H. Song, H.R. Wang, Y.Q. Yang, et al., J. Mater. Sci. Mater. Med. 29 (2018) 1-11.
C. Li, D.Y. Lu, J.J. Deng, X. Zhang, P. Yang, Adv. Mater. 31 (2019) e1903973. doi: 10.1002/adma.201903973
S. Srinivasan, R. Jayasree, K.P. Chennazhi, S.V. Nair, R. Jayakumar, Carbohydr. Polym. 87 (2012) 274-283. doi: 10.1016/j.carbpol.2011.07.058
H. Autefage, F. Allen, H.M. Tang, et al., Biomaterials 209 (2019) 152-162. doi: 10.1016/j.biomaterials.2019.03.035
W. Niu, M. Chen, Y. Guo, et al., ACS Nano 15 (2021) 14323-14337. doi: 10.1021/acsnano.1c03214
S. Kargozar, F. Baino, S. Hamzehlou, R.G. Hill, M. Mozafari, Trends Biotechnol. 36 (2018) 430-444. doi: 10.1016/j.tibtech.2017.12.003
K. Sawant, A.M. Pawar, Saudi J. Oral Sci. 7 (2020) 3-10. doi: 10.4103/sjos.SJOralSci_56_19
X.Y. Sheng, W.Y. Gong, Q. Hu, X.F. Chen, Y.M. Dong, Chin. Chem. Lett. 27 (2016) 1509-1514. doi: 10.1016/j.cclet.2016.03.030
A.R. Curtis, N.X. West, B. Su, Acta Biomater. 6 (2010) 3740-3746. doi: 10.1016/j.actbio.2010.02.045
J.C. Mitchell, L. Musanje, J.L. Ferracane, Dent. Mater. 27 (2011) 386-393. doi: 10.1016/j.dental.2010.11.019
E. Lynch, D.S. Brauer, N. Karpukhina, D.G. Gillam, R.G. Hill, Dent. Mater. 28 (2012) 168-178. doi: 10.1016/j.dental.2011.11.021
T.C.C. Lopez, I.M.A. Diniz, L.S. Ferreira, et al., J. Biomed. Mater. Res., Part B 105 (2017) 107-116. doi: 10.1002/jbm.b.33532
Y.C. Chiang, H.P. Lin, H.H. Chang, et al., ACS Nano 8 (2014) 12502-12513. doi: 10.1021/nn5053487
M.A. Malkoç, M. Sevimay, Lasers Med. Sci. 27 (2012) 743-748. doi: 10.1007/s10103-011-0954-6
M.M. Moreira, L.R.R. d. Silva, T.A.D. Mendes, et al., Dent. Mater. 34 (2018) 1144-1153. doi: 10.1016/j.dental.2018.04.011
P. Schüpbach, F. Lutz, W.J. Finger, Eur. J. Oral Sci. 105 (1997) 414-421. doi: 10.1111/j.1600-0722.1997.tb02138.x
A. Bechir, V. Hancu, G. Ciavoi, et al., Acta Stomatol. Marisiensis 1 (2018) 74-81.
Y. Zhou, M. Yang, Q.J. Jia, et al., ACS Omega 6 (2021) 19596-19605. doi: 10.1021/acsomega.1c02123
B. Allard, H. Magloire, M.L. Couble, J.C. Maurin, F. Bleicher, J. Biol. Chem. 281 (2006) 29002-29010. doi: 10.1074/jbc.M601020200
A. Alloui, K. Zimmermann, J. Mamet, et al., EMBO J. 25 (2006) 2368-2376. doi: 10.1038/sj.emboj.7601116
M.Z. Hossain, M.M. Bakri, F. Yahya, et al., Int. J. Mol. Sci. 20 (2019) 526-556. doi: 10.3390/ijms20030526
X. Liu, C. Wang, T. Fujita, et al., J. Dent. Res. 94 (2015) 1259-1266. doi: 10.1177/0022034515592858
J.J. Ryu, S. Yoo, K.Y. Kim, et al., J. Dent. Res. 89 (2010) 1455-1460. doi: 10.1177/0022034510381394
B.B. Lier, C.K. Rösing, A.M. Aass, P. Gjermo, J. Clin. Periodontol. 29 (2002) 501-506. doi: 10.1034/j.1600-051X.2002.290605.x
Y. Kimura, P. Wilder-Smith, K. Yonaga, K. Matsumoto, J. Clin. Periodontol. 27 (2000) 715-721. doi: 10.1034/j.1600-051x.2000.027010715.x
S.M. Al-Qahtani, Open Access Maced. J. Med. Sci. 7 (2019) 1685-1690. doi: 10.3889/oamjms.2019.344
S.M.A. Silva, J. Malacarne-Zanon, R.M. Carvalho, et al., Oper. Dent. 37 (2012) 356-362. doi: 10.2341/09-228-L
D.G. Gillam, N. Khan, N.J. Maidan, P.M. Barbe, Dent. Traumatol. 15 (1999) 198-204. doi: 10.1111/j.1600-9657.1999.tb00774.x
A.C. Machado, F.E.M. Rabelo, V. Maximiano, et al., J. Dent. 86 (2019) 53-59. doi: 10.1016/j.jdent.2019.05.025
N. Wara-aswapati, D. Krongnawakul, D. Jiraviboon, et al., J. Clin. Periodontol. 32 (2005) 53-58. doi: 10.1111/j.1600-051X.2004.00631.x
E. Zarzecka-Francica, J. Golda, O. Gornicka, et al., Folia Med. Cracov. 2 (2020) 43-54.
P. Amini, M. Miner, P.A. Sagel, R.W. Gerlach, Compend. Contin. Educ. Dent. 37 (2016) e21-e25.
J.M. Peacock, R. Orchardson, J. Clin. Periodontol. 26 (1999) 33-37. doi: 10.1034/j.1600-051x.1999.260106.x
K. McCormack, R. Davies, Pain 68 (1996) 5-11. doi: 10.1016/S0304-3959(96)03142-9
M.F. Cuenin, M.J. Scheidt, R.B. O'Neal, et al., J. Clin. Periodontol. 62 (1991) 668-673. doi: 10.1902/jop.1991.62.11.668

Scheme 1 DH desensitization therapy involves various biomaterials to achieve dentinal tubule closure and dental nerve blockade.

Figure 1 Dentin desensitizing agent mediated by TA/Fe3+ complex. (A) TA/Fe3+ complex to seal dentinal tubules. (B) Evaluation method of dentinal tubule permeability. (C, D) Dentinal permeability assessment under 200 mm H2O for 600 s after TA/Fe3+ and GlumaⓇ treatment. (E) Energy dispersive spectroscopy of HA mineralization on dentin slice after TA/Fe3+ treatment. (F) Human periodontal ligament (hPDL) tissue. (G, H) Assessing hPDL cell adhesion and proliferation on TA/Fe3+-coated and HA-remineralized cell culture dishes. NS = not significant (P > 0.05). P < 0.05. Reproduced with permission [81]. Copyright 2015. The author(s).

Figure 2 Dentinal remineralization of LYZ-PEG nanofilm. (A) LYZ-PEG-mediated dentinal remineralization. (B) Energy dispersive X-ray (EDX) spectrum of remineralization layer after applying LYZ-PEG. (C) XRD results of dentin, ethylene diamine tetraacetic acid (EDTA)-etched dentin, and remineralization layer. (D) Results of air pressure tests of dentin samples with different treatments. (E) Air pressure infiltration apparatus. (F) Antifouling surface of LYZ-PEG nanofilm. Reproduced with permission [87]. Copyright 2019, John Wiley & Sons.

 扫一扫看文章
扫一扫看文章

扫一扫关注我们
 DownLoad:
DownLoad:
 下载:
下载:
 下载:
下载: